Download
1 / 42
430 likes | 946 Views
Medical Nutrition Therapy for Liver, Biliary System, and Exocrine Pancreas Disorders. Relationship of Organs of the Upper Abdomen. A, Liver (retracted upward); B, gallbladder; C, esophageal opening of the stomach; D, stomach (shown in dotted outline); E, common

E N D
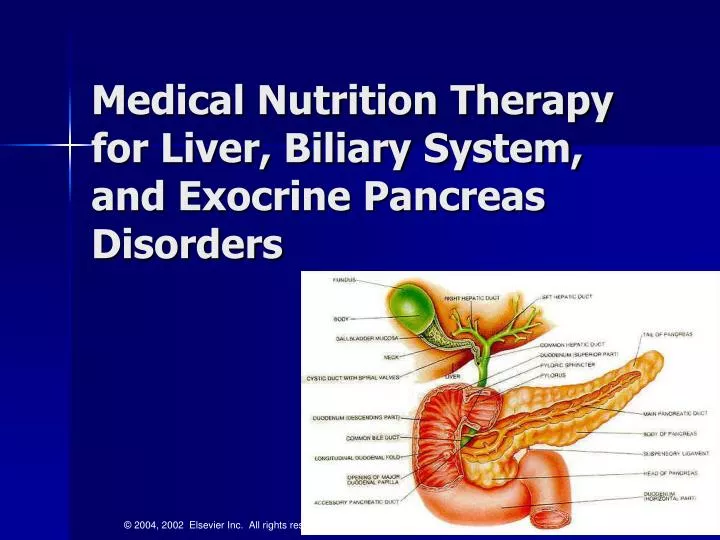
Medical Nutrition Therapy for Liver, Biliary System, and Exocrine Pancreas Disorders
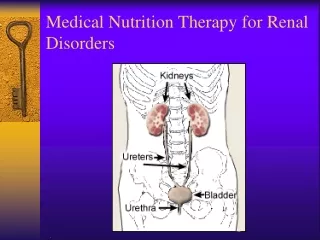
Relationship of Organs of the Upper Abdomen A, Liver (retracted upward); B, gallbladder; C, esophageal opening of the stomach; D, stomach (shown in dotted outline); E, common bile duct; F, duodenum; G, pancreas and pancreatic duct; H, spleen; I, kidneys. Courtesy The Cleveland Clinic Foundation, Cleveland, Ohio, 2002.
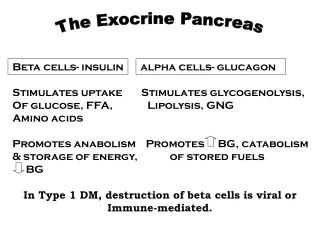
The Liver • Largest gland in the body (about 1500 g) • Essential for life, though survival is possible with 10-20% function • Plays major role in macronutrient and micronutrient digestion, metabolism, and storage • Metabolizes steroids, detoxifies drugs, alcohol, ammonia
Diseases of the Liver • Acute viral hepatitis • Fulminant hepatitis • Chronic hepatitis • Alcoholic liver disease, alcoholic hepatitis, and cirrhosis • Non-alcoholic hepatic steatosis (NASH)
Diseases of the Liver • Cholestatic liver diseases —Primary biliary cirrhosis —Sclerosing cholangitis • Inherited disorders • Other liver diseases
Acute Viral Hepatitis • Widespread inflammation of the liver that is caused by hepatitis viruses A, B, C, D and E • Hep A: oral-fecal route • Hep B and C: body fluids • Hep D: occurs only in pts with Hep B • Hep E: oral-fecal route; seen more often in Asia, Africa, Mexico Hasse JM et al. ASPEN Nutrition Support Practice Manual, 2nd edition, 2005
Acute Viral Hepatitis • Four phases of symptoms: 1. Prodromal phase 2. Preicteric phase 3. Icteric phase 4. Convalescent phase
Risk Factors for Chronic Viral Hepatitis • Injection drug use • Chronic hemodialysis • Blood transfusion or transplantation prior to 1992 (HCV) • Receipt of blood (including needlestick) from a donor subsequently testing positive for HCV
Risk Factors for Chronic Viral Hepatitis • Receipt of clotting factor concentrates produced before 1987 • Asian ancestry (HBV) • Unvaccinated health care workers • Birth to mother with chronic HBV or HCV
Possible Risk Factors • Body piercing or tattooing • Multiple sexual partners or sexually transmitted diseases • Health care workers (HCV) • Contacts of HCV positive persons Source: NACB Laboratory Guidelines for Screening, Diagnosis, and Monitoring of Hepatic Injury. Dufour, Lott, Nolte, Gretch, Koff, Seeff
Fulminant Hepatitis • Syndrome in which severe liver dysfunction is accompanied by hepatic encephalopathy within 8 weeks • Causes include viral hepatitis (75%), chemical toxicity (acetaminophen, drug reactions, poisonous mushrooms, other poisons) • Complications include cerebral edema, coagulopathy, bleeding, cardiovascular complications, renal failure, pancreatitis
Chronic Hepatitis • At least 6-month course of hepatitis or biochemical and clinical evidence of liver disease with confirmatory biopsy findings of unresolving hepatic inflammation • Can be caused by autoimmune, viral, metabolic, or toxic etiologies
Alcoholic Liver Disease: Most Common Liver Disease • Alcohol excess and abuse • Most common cause of liver disease in the U.S. • Fourth leading cause of death among middle-aged Americans • Alcohol problems are highest among young adults, ages 18 to 29.
Stages of Alcoholic Liver Disease • Hepatic steatosis • Alcoholic hepatitis • Alcoholic (Leannec’s) cirrhosis
Microscopic Image of (A) Normal Liver; (B) cirrhotic liver) (Adapted from Bray GA. Gray DS, Obesity, part 1: Pathogenisis. West J Med 149:429, 1988; and Lew EA, Garfinkle L; Variations in mortality by weight among 750,000 men and women. J Clin Epidemiol 32:563, 1979.) (From Kanel G, Korula J. Atlas of Liver Pathology. W.B. Saunders, 1992.)
Liver Test Panel • Aspartate transaminase (AST) • Alanine aminotransferase (ALT) • Alkaline phosphatase (ALP) • Total bilirubin • Direct bilirubin • PT/PTT • Ceruloplasmin • Total protein • Albumin • Viral serologies
Lab Tests in Acute Liver Disease *upper reference limit Source: NACB Laboratory guidelines for screening, diagnosis, and monitoring of hepatic injury. Dufour, Lou, Nolic, Gretch, Koff, Seeff
Causes of Elevated ALT and/or AST Source: NACB Laboratory guidelines for screening, diagnosis, and monitoring of hepatic injury. Dufour, Lou, Nolic, Gretch, Koff, Seeff
Body weight Anthropometric measurements Creatinine-height index Nitrogen balance studies Visceral protein levels Immune function tests Interpretation of Nutrition Assessment Tests in Patients with End-Stage Liver Disease
Causes of Malnutrition in Liver Disease • Anorexia • Early satiety or dysgeusia • Nausea and vomiting • Maldigestion or malabsorption • Restricted diets • Altered metabolism
Malnutrition in Liver Disease—Pathophysiology Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Jeanette M. Hasse and Laura E. Matarese, 2002.
Malnutrition in Liver Disease—Medical and Nutritional Management Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Jeanette M. Hasse and Laura E. Matarese, 2002.
Vitamin A Vitamin D Vitamin E Vitamin K Vitamin B6 Vitamin B12 Folate Niacin Thiamin Zinc Magnesium Iron Potassium Phosphorus Vitamin/Mineral Deficits* in Severe Hepatic Failure * May be related to fat malabsorption, medications, alcoholism (p. 752 Krause)
Four Stages of Hepatic Encephalopathy StageSymptom I Mild confusion, agitation, irritability, sleep disturbance, decreased attention II Lethargy, disorientation, inappropriate behavior, drowsiness III Somnolence but arousable, incomprehensible speech, confusion, aggression when awake IV Coma
Relationship of Organs of the Upper Abdomen A, Liver (retracted upward); B, gallbladder; C, esophageal opening of the stomach; D, stomach (shown in dotted outline); E, common bile duct; F, duodenum; G, pancreas and pancreatic duct; H, spleen; I, kidneys. Courtesy The Cleveland Clinic Foundation, Cleveland, Ohio, 2002.
Choledocholithiasis http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/17038.jpg
Pancreatitis http://www.pennhealth.com/health_info/Surgery/pancreatitis_2.html
Acute Hemorrhagic Pancreatitis http://www.pathguy.com/~lulo/lulo0028.htm
Acute Pancreatitis • 75% alcohol related • 15% related to gallstones • 10% trauma, hyperlipidemia, hypercalcemia, medications, etc. Mascarenhas et al. ASPEN Nutrition Support Practice Manual, 2nd edition, 2005, p. 211
Whipple Procedure Source: Johns Hopkins http://www.hopkins-gi.org/pages/latin/templates/ index.cfm?pg=disease3&organ=4&disease =24&lang_id=1&pagetype=12&pagenum=263
MNT in Liver/Biliary Disease • Disease of the liver/biliary tract has a profound effect on digestion and absorption • Often leads to malnutrition; malnutrition exacerbates effect of disease • Appropriate nutrition care is key in reducing associated morbidity and mortality and improving quality of life