Download
1 / 1
10 likes | 133 Views
Increased Mortality in Rural Patients with HIV in New England Timothy Lahey 1, 2 ; Michelle Lin 1 ; Bryan Marsh 2 ; Jim Curtin 2 ; Kim Wood 2 ; Betsy Eccles 1,2 ; C. Fordham von Reyn 1,2 Dartmouth Medical School 1 and Dartmouth-Hitchcock Medical Center 2 , Lebanon, NH 03756. Background.

E N D
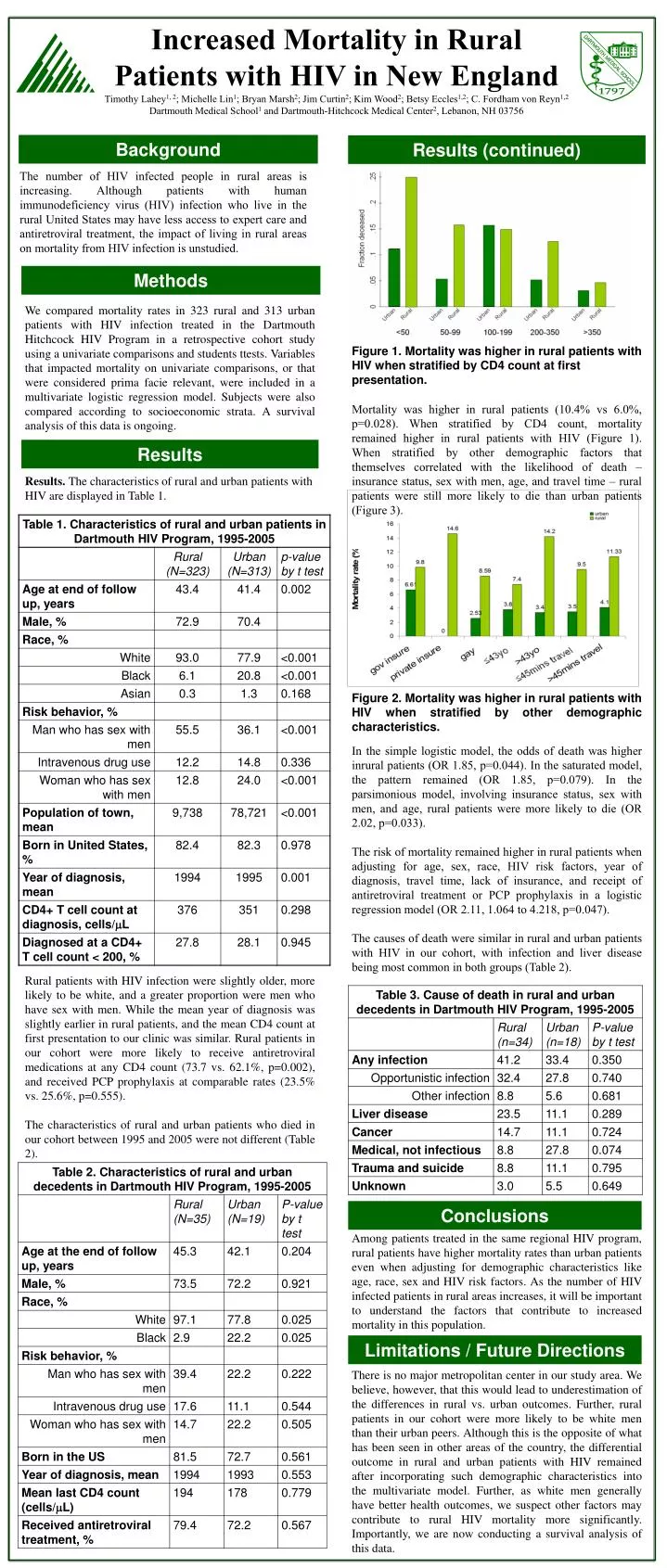
Increased Mortality in Rural Patients with HIV in New England Timothy Lahey1, 2; Michelle Lin1; Bryan Marsh2; Jim Curtin2; Kim Wood2; Betsy Eccles1,2; C. Fordham von Reyn1,2 Dartmouth Medical School1 and Dartmouth-Hitchcock Medical Center2, Lebanon, NH 03756 Background Results (continued) The number of HIV infected people in rural areas is increasing. Although patients with human immunodeficiency virus (HIV) infection who live in the rural United States may have less access to expert care and antiretroviral treatment, the impact of living in rural areas on mortality from HIV infection is unstudied. Methods We compared mortality rates in 323 rural and 313 urban patients with HIV infection treated in the Dartmouth Hitchcock HIV Program in a retrospective cohort study using a univariate comparisons and students ttests. Variables that impacted mortality on univariate comparisons, or that were considered prima facie relevant, were included in a multivariate logistic regression model. Subjects were also compared according to socioeconomic strata. A survival analysis of this data is ongoing. Figure 1. Mortality was higher in rural patients with HIV when stratified by CD4 count at first presentation. Mortality was higher in rural patients (10.4% vs 6.0%, p=0.028). When stratified by CD4 count, mortality remained higher in rural patients with HIV (Figure 1). When stratified by other demographic factors that themselves correlated with the likelihood of death – insurance status, sex with men, age, and travel time – rural patients were still more likely to die than urban patients (Figure 3). Results Results. The characteristics of rural and urban patients with HIV are displayed in Table 1. Figure 2. Mortality was higher in rural patients with HIV when stratified by other demographic characteristics. In the simple logistic model, the odds of death was higher inrural patients (OR 1.85, p=0.044). In the saturated model, the pattern remained (OR 1.85, p=0.079). In the parsimonious model, involving insurance status, sex with men, and age, rural patients were more likely to die (OR 2.02, p=0.033). The risk of mortality remained higher in rural patients when adjusting for age, sex, race, HIV risk factors, year of diagnosis, travel time, lack of insurance, and receipt of antiretroviral treatment or PCP prophylaxis in a logistic regression model (OR 2.11, 1.064 to 4.218, p=0.047). The causes of death were similar in rural and urban patients with HIV in our cohort, with infection and liver disease being most common in both groups (Table 2). Rural patients with HIV infection were slightly older, more likely to be white, and a greater proportion were men who have sex with men. While the mean year of diagnosis was slightly earlier in rural patients, and the mean CD4 count at first presentation to our clinic was similar. Rural patients in our cohort were more likely to receive antiretroviral medications at any CD4 count (73.7 vs. 62.1%, p=0.002), and received PCP prophylaxis at comparable rates (23.5% vs. 25.6%, p=0.555). The characteristics of rural and urban patients who died in our cohort between 1995 and 2005 were not different (Table 2). Conclusions Among patients treated in the same regional HIV program, rural patients have higher mortality rates than urban patients even when adjusting for demographic characteristics like age, race, sex and HIV risk factors. As the number of HIV infected patients in rural areas increases, it will be important to understand the factors that contribute to increased mortality in this population. There is no major metropolitan center in our study area. We believe, however, that this would lead to underestimation of the differences in rural vs. urban outcomes. Further, rural patients in our cohort were more likely to be white men than their urban peers. Although this is the opposite of what has been seen in other areas of the country, the differential outcome in rural and urban patients with HIV remained after incorporating such demographic characteristics into the multivariate model. Further, as white men generally have better health outcomes, we suspect other factors may contribute to rural HIV mortality more significantly. Importantly, we are now conducting a survival analysis of this data. Limitations / Future Directions






















