Download
1 / 1
10 likes | 119 Views
Benign Fibroepithelial Polyps: A Rare Cause of Ureteropelvic Junction Obstruction in Children. Anitha Ezekiel, M.D. Driscoll Children’s Hospital- Corpus Christi, PGY 1. Abstract. Results.

E N D
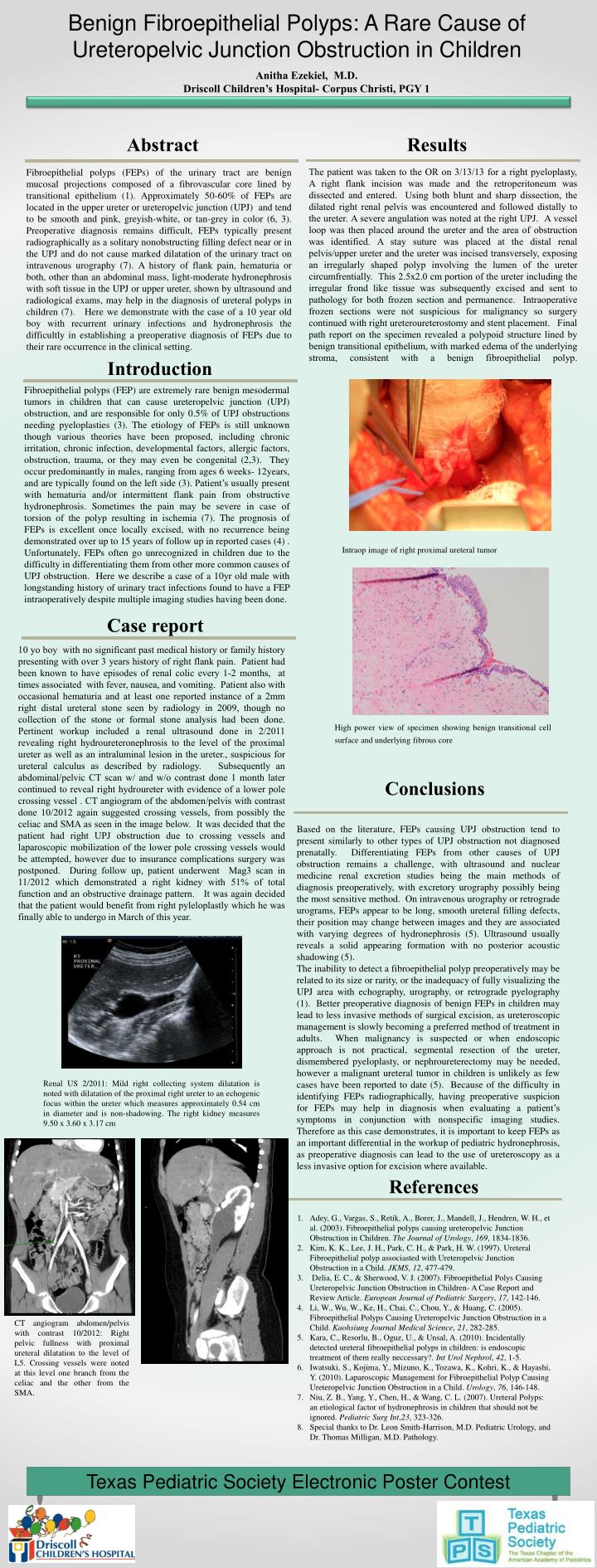
Benign Fibroepithelial Polyps: A Rare Cause of Ureteropelvic Junction Obstruction in Children Anitha Ezekiel, M.D. Driscoll Children’s Hospital- Corpus Christi, PGY 1 Abstract Results The patient was taken to the OR on 3/13/13 for a right pyeloplasty, A right flank incision was made and the retroperitoneum was dissected and entered. Using both blunt and sharp dissection, the dilated right renal pelvis was encountered and followed distally to the ureter. A severe angulation was noted at the right UPJ. A vessel loop was then placed around the ureter and the area of obstruction was identified. A stay suture was placed at the distal renal pelvis/upper ureter and the ureter was incised transversely, exposing an irregularly shaped polyp involving the lumen of the ureter circumfrentially. This 2.5x2.0 cm portion of the ureter including the irregular frond like tissue was subsequently excised and sent to pathology for both frozen section and permanence. Intraoperative frozen sections were not suspicious for malignancy so surgery continued with right ureteroureterostomy and stent placement. Final path report on the specimen revealed a polypoid structure lined by benign transitional epithelium, with marked edema of the underlying stroma, consistent with a benign fibroepithelial polyp. Fibroepithelial polyps (FEPs) of the urinary tract are benign mucosal projections composed of a fibrovascular core lined by transitional epithelium (1). Approximately 50-60% of FEPs are located in the upper ureter or ureteropelvic junction (UPJ) and tend to be smooth and pink, greyish-white, or tan-grey in color (6, 3). Preoperative diagnosis remains difficult, FEPs typically present radiographically as a solitary nonobstructing filling defect near or in the UPJ and do not cause marked dilatation of the urinary tract on intravenous urography (7). A history of flank pain, hematuria or both, other than an abdominal mass, light-moderate hydronephrosis with soft tissue in the UPJ or upper ureter, shown by ultrasound and radiological exams, may help in the diagnosis of ureteral polyps in children (7). Here we demonstrate with the case of a 10 year old boy with recurrent urinary infections and hydronephrosis the difficultly in establishing a preoperative diagnosis of FEPs due to their rare occurrence in the clinical setting. Introduction Fibroepithelial polyps (FEP) are extremely rare benign mesodermal tumors in children that can cause ureteropelvic junction (UPJ) obstruction, and are responsible for only 0.5% of UPJ obstructions needing pyeloplasties (3). The etiology of FEPs is still unknown though various theories have been proposed, including chronic irritation, chronic infection, developmental factors, allergic factors, obstruction, trauma, or they may even be congenital (2,3). They occur predominantly in males, ranging from ages 6 weeks- 12years, and are typically found on the left side (3). Patient’s usually present with hematuria and/or intermittent flank pain from obstructive hydronephrosis. Sometimes the pain may be severe in case of torsion of the polyp resulting in ischemia (7). The prognosis of FEPs is excellent once locally excised, with no recurrence being demonstrated over up to 15 years of follow up in reported cases (4) . Unfortunately, FEPs often go unrecognized in children due to the difficulty in differentiating them from other more common causes of UPJ obstruction. Here we describe a case of a 10yr old male with longstanding history of urinary tract infections found to have a FEP intraoperatively despite multiple imaging studies having been done. Intraop image of right proximal ureteral tumor Case report 10 yo boy with no significant past medical history or family history presenting with over 3 years history of right flank pain. Patient had been known to have episodes of renal colic every 1-2 months, at times associated with fever, nausea, and vomiting. Patient also with occasional hematuria and at least one reported instance of a 2mm right distal ureteral stone seen by radiology in 2009, though no collection of the stone or formal stone analysis had been done. Pertinent workup included a renal ultrasound done in 2/2011 revealing right hydroureteronephrosis to the level of the proximal ureter as well as an intraluminal lesion in the ureter., suspicious for ureteral calculus as described by radiology. Subsequently an abdominal/pelvic CT scan w/ and w/o contrast done 1 month later continued to reveal right hydroureter with evidence of a lower pole crossing vessel . CT angiogram of the abdomen/pelvis with contrast done 10/2012 again suggested crossing vessels, from possibly the celiac and SMA as seen in the image below. It was decided that the patient had right UPJ obstruction due to crossing vessels and laparoscopic mobilization of the lower pole crossing vessels would be attempted, however due to insurance complications surgery was postponed. During follow up, patient underwent Mag3 scan in 11/2012 which demonstrated a right kidney with 51% of total function and an obstructive drainage pattern. It was again decided that the patient would benefit from right pyleloplastly which he was finally able to undergo in March of this year. High power view of specimen showing benign transitional cell surface and underlying fibrous core Conclusions Based on the literature, FEPs causing UPJ obstruction tend to present similarly to other types of UPJ obstruction not diagnosed prenatally. Differentiating FEPs from other causes of UPJ obstruction remains a challenge, with ultrasound and nuclear medicine renal excretion studies being the main methods of diagnosis preoperatively, with excretory urography possibly being the most sensitive method. On intravenous urography or retrograde urograms, FEPs appear to be long, smooth ureteral filling defects, their position may change between images and they are associated with varying degrees of hydronephrosis (5). Ultrasound usually reveals a solid appearing formation with no posterior acoustic shadowing (5). The inability to detect a fibroepithelial polyp preoperatively may be related to its size or rarity, or the inadequacy of fully visualizing the UPJ area with echography, urography, or retrograde pyelography (1). Better preoperative diagnosis of benign FEPs in children may lead to less invasive methods of surgical excision, as ureteroscopic management is slowly becoming a preferred method of treatment in adults. When malignancy is suspected or when endoscopic approach is not practical, segmental resection of the ureter, dismembered pyeloplasty, or nephroureterectomy may be needed, however a malignant ureteral tumor in children is unlikely as few cases have been reported to date (5). Because of the difficulty in identifying FEPs radiographically, having preoperative suspicion for FEPs may help in diagnosis when evaluating a patient’s symptoms in conjunction with nonspecific imaging studies. Therefore as this case demonstrates, it is important to keep FEPs as an important differential in the workup of pediatric hydronephrosis, as preoperative diagnosis can lead to the use of ureteroscopy as a less invasive option for excision where available. Renal US 2/2011: Mild right collecting system dilatation is noted with dilatation of the proximal right ureter to an echogenic focus within the ureter which measures approximately 0.54 cm in diameter and is non-shadowing. The right kidney measures 9.50 x 3.60 x 3.17 cm References Adey, G., Vargas, S., Retik, A., Borer, J., Mandell, J., Hendren, W. H., et al. (2003). Fibroepithelial polyps causing ureteropelvic Junction Obstruction in Children. The Journal of Urology, 169, 1834-1836. Kim, K. K., Lee, J. H., Park, C. H., & Park, H. W. (1997). Ureteral Fibroepithelial polyp associasted with Ureteropelvic Junction Obstruction in a Child. JKMS, 12, 477-479. Delia, E. C., & Sherwood, V. J. (2007). Fibroepithelial Polys Causing Ureteropelvic Junction Obstruction in Children- A Case Report and Review Article. European Journal of Pediatric Surgery, 17, 142-146. Li, W., Wu, W., Ke, H., Chai, C., Chou, Y., & Huang, C. (2005). Fibroepithelial Polyps Causing Ureteropelvic Junction Obstruction in a Child. Kaohsiung Journal Medical Science, 21, 282-285. Kara, C., Resorlu, B., Oguz, U., & Unsal, A. (2010). Incidentally detected ureteral fibroepithelial polyps in children: is endoscopic treatment of them really neccessary?. Int Urol Nephrol, 42, 1-5. Iwatsuki, S., Kojima, Y., Mizuno, K., Tozawa, K., Kohri, K., & Hayashi, Y. (2010). Laparoscopic Management for Fibroepithelial Polyp Causing Ureteropelvic Junction Obstruction in a Child. Urology, 76, 146-148. Niu, Z. B., Yang, Y., Chen, H., & Wang, C. L. (2007). Ureteral Polyps: an etiological factor of hydronephrosis in children that should not be ignored. Pediatric Surg Int,23, 323-326. Special thanks to Dr. Leon Smith-Harrison, M.D. Pediatric Urology, and Dr. Thomas Milligan, M.D. Pathology. CT angiogram abdomen/pelvis with contrast 10/2012: Right pelvic fullness with proximal ureteral dilatation to the level of L5. Crossing vessels were noted at this level one branch from the celiac and the other from the SMA. Texas Pediatric Society Electronic Poster Contest



















