Download
1 / 30
330 likes | 604 Views
By : Nour Eldin Mohammed Ref: Khaled M. Elsayes, et al , 2004, Radiographics. Adrenal Masses: MR Imaging Features with Pathologic Correlation. Normal Anatomy .

E N D
By : Nour Eldin Mohammed Ref: Khaled M. Elsayes, et al , 2004, Radiographics Adrenal Masses: MR Imaging Features with Pathologic Correlation
Normal Anatomy • The adrenal glands are two small, yellowish bodies located in the perirenal space, immediately anterosuperior to the upper pole of the kidneys. • They are very vascular and receive blood supply from the superior, middle, and inferior suprarenal arteries
The adrenal gland is composed of an outer cortex and thinner inner medulla. • The cortex is further subdivided into three zones: outer zona glomerulosa, middle zona fasciculata, and inner zona reticularis
Normal MRI Appearance • The right adrenal gland is located posterior to the inferior vena cava and superior to the upper pole of the right kidney. • The left adrenal gland is anteromedial to the upper pole of the kidney and posterior to the pancreas • Normal adrenal glands range from 2 to 6 mm in thickness and from 2 to 4 cm in length
Fat-containing Adrenal Masses • Fat-containing adrenal masses can be classified into two main types: • those that contain intracellular fat (eg, adenoma) • and those with macroscopic fat (eg, myelolipoma).
Adrenal Adenoma • The most common adrenal lesions. • Characterised by the presence of intracellular lipid. • Chemical shift imaging is the most reliable technique for diagnosing adrenal adenoma with loss of signal intensity on out-of-phase images. • Uniform enhancement with contrast enhanced images is typical of adenomas. • Cystic changes, hemorrhage, or variation in vascularity lead to small, rounded foci of altered signal intensity.
Axial in Phase MRI Axial out of phase MRI
Myelolipoma • The myelolipoma is an uncommon benign tumor composed of mature adipose tissue and hematopoietic tissue. • Mostly discovered accidentally. • The fatty component of this tumor is hyperintense on T1-weighted images. • With loss of signal intensity of the fatty component on Fat-Suppressed Technique.
Axial T1 with Fat Suppressed Technique Axial T1 MRI
Cystic Masses • These include : • Simple Cysts • Pseudocysts • Lymphangioma
Simple Cysts T1 Coronal MRI T2 Coronal MRI
Pseudocysts • Pseudocysts typically arise after an episode of adrenal hemorrhage and do not have an epithelial lining. • Have a complicated appearance on MR images, manifesting with septations, blood products, or a soft-tissue component secondary to hemorrhage or hyalinized thrombus. • Peripheral curvilinear calcification may be present.
Coronal T2 MRI Axial T1 with Contrast
Lymphangioma Low signal intensity at T1-weighted imaging and high signal intensity at T2-weighted
Hypervascular Lesions (Pheochromocytoma) • It arises from the adrenal medulla. • 10% of pheochromocytomas are bilateral,10% are extraadrenal,10% occur in children, and 10% are malignant • Pheochromocytomas do not contain a substantial amount of cytoplasmic lipid, So they maintain their signal intensity on out-of-phase GRE chemical shift images. • Most pheochromocytomas demonstrate high signal intensity on T2-weighted images (light bulb sign).
Axial T1 in Phase MRI Axial T1 out of Phase MRI Contrast-enhanced Image
Malignant Neoplasms • Adrenocortical Carcinoma • Adrenal Lymphoma • Metastases
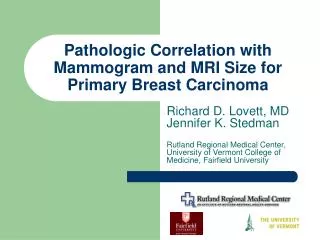
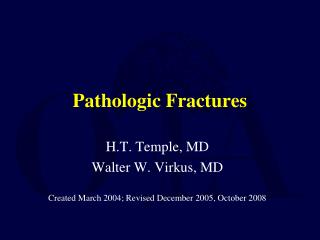
Adrenocortical Carcinoma • a rare tumor. • Age : 30 - 70 • Large size • Can manifest as a hyperfunctioning mass causing Cushing syndrome or Conn syndrome. • Other manifestations include an abdominal mass and abdominal pain.
Sagittal 3D contrast-enhanced MRI Coronal T2-weighted MRI
Adrenal Lymphoma • More with non-Hodgkin lymphoma • Bilateral involvement occurs in 50% of patients . • Characterized by low signal intensity on T1 WI and heterogeneous high signal intensity on T2 WI , with minimal progressive enhancement after administration of contrast material.
Axial T1-weighted MRI Axial T2-weighted MRI
Metastases • The most common malignant lesions involving the adrenal gland. • Found in up to 27% of patients with Carcinomas at autopsy. • Common primary sites of tumors that metastasize to the adrenal glands include the lung, bowel, breast, and pancreas. • Usually bilateral but may also be unilateral.
Contrast Enhanced T1 Image Of Metastatic Deposit From Renal Cell Carcinoma
Pediatric Neoplasms • Neuroblastoma • Ganglioneuroblastoma
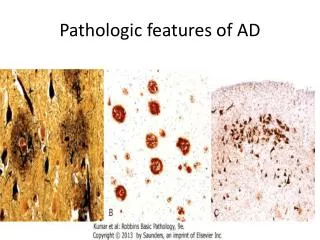
Neuroblastoma • The 2nd most common pediatric abdominal mass (after Wilms tumor). • Representing 5%–15% of all malignant tumors in children . • Arises from the neural crest in the adrenal medulla or along the sympathetic chain. • Usually demonstrates heterogeneous low signal intensity on T1-weighted images, high signal intensity on T2-weighted images , and enhancement after administration of contrast material. • Calcification is present in 80%–90% of the lesions
Coronal unenhanced T1 MRI Axial T2 MRI
Ganglioneuroblastoma • Intermediate in malignancy between that of neuroblastoma and ganglioneuroma • arise from the neural crest. • Ganglioneuroblastoma are smaller and more well defined than neuroblastoma • Demonstrates Intermediate signal intensity on T1 WI and heterogeneously high signal intensity on T2 WI, with heterogeneous enhancement after administration of contrast material.
T1-WI shows a heterogeneous mass with intermediate signal intensity