Download
1 / 33
330 likes | 523 Views
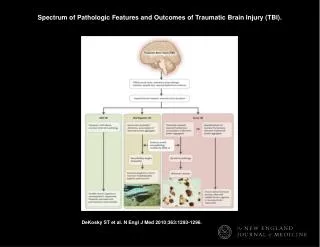
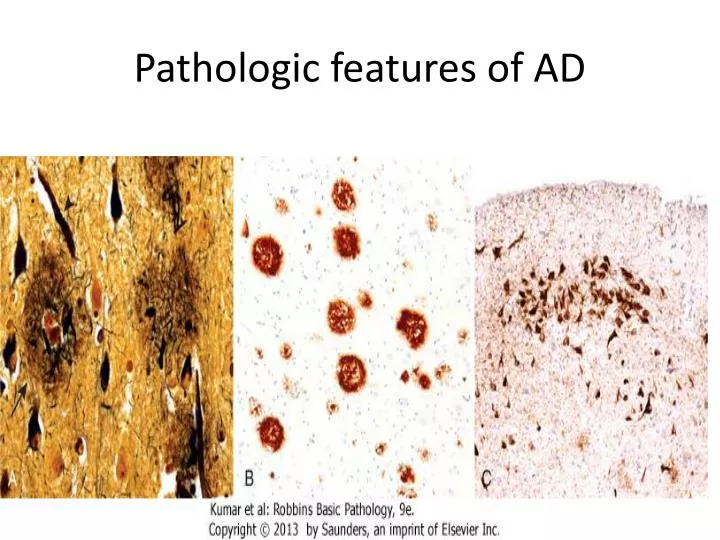
Pathologic features of AD. Pathologic changes (specifically plaques, tangles, and the associated neuronal loss and glial reaction) a. Are evident first in the entorhinal cortex b. Then in the hippocampal formation, c. And finally in the neocortex . . Neuritic plaques :

E N D
Pathologic changes (specifically plaques, tangles, and the associated neuronal loss and glial reaction) a. Are evident first in the entorhinal cortex b. Then in the hippocampal formation, c. And finally in the neocortex.
Neuritic plaques : • Are focal, spherical collections of dilated, tortuous, silver-staining neuritic processes (dystrophic neurites), often around a central amyloid core • Range in size from 20 to 200 μm in diameter - Plaques can be found in the hippocampus and amygdala as well as in the neocortex
- There usually is relative sparing of primary motor and sensory cortices until late in the disease course. 2. Diffuse plaques: - Are Aβ deposits lacking the surrounding neuritic reaction, typically are found in the superficial cerberal cortex, basal ganglia , and the cerebellar cortex
2..Neurofibrillary tangles : - Are bundles of paired helical filaments visible as basophilic in the cytoplasm of the neurons that displace or encircle the nucleus; - Tangles can persist after neurons die, becoming a form of extracellular pathology and are commonly found in:
a. In the entorhinal cortex, b. In pyramidal cells of the hippocampus and amygdala, • The basal forebrain, and the raphe nuclei. - A major component of paired helical filaments is abnormally hyperphosphorylatedtau - Tangles are not specific to AD, being found in other degenerative diseases as well
II. Frontotemporal Lobar Degeneration • These disorders share clinical features - Progressive deterioration of language and personality changes stemming from the degeneration of temporal and frontal lobes; and are referred to as frontotemporal dementias. 1. When the frontal lobe bears the greatest burden of disease, behavioral changes often dominate, 2. Whereas when the disease begins in the temporal lobe, language problems often are the presenting complaint
- These symptoms precede memory disturbances, which can assist in their separation from AD on clinical grounds. On gross inspection : There is atrophy of the brain that predominantly affects the frontal and temporal lobes Note; Different subgroups are characterized by neuronal inclusions involving the affected regions. a. In some cases the defining inclusions contain tau (FTLD-tau), but the configuration of the tau inclusions differs from the tau-containing tangles of AD.
- FTLD-tau sometimes is caused by mutations in the gene encoding tau. • One well-recognized subtype of FTLD-tau is Pick disease, which is associated with smooth, round inclusions known as Pick bodies. b. The other major form of FTLD is characterized by aggregates containing the TDP-43 (FTLD-TDP43). - This form of FTLD is associated with predominantly frontal lobe cognitive impairment and it is sometimes caused by mutations in the gene encoding TDP-43,
III. Parkinson Disease - Parkinsonism is a clinical syndrome characterized by tremor, rigidity, bradykinesia and instability. - These types of motor disturbances may be seen in a range of diseases that damage dopaminergic neurons, which project from the substantianigra to the striatum. - It can be induced by drugs such as dopamine antagonists or toxins that selectively injure dopaminergic neurons.
- Most cases of parkinsonism are caused by idiopathic Parkinson disease (PD) but other diseases in which parkinsonism may be present and include:- 1. Multiple system atrophy (MSA) 2. Progressive supranuclear palsy (PSP) 3. Corticobasal degeneration (CBD), 4. Postencephalitic parkinsonism, which was associated with the 1918 influenza pandemic.
PATHOGENESIS OF IDIOPATHIC PARKINSON DISEASE - Most cases are sporadic, but both autosomal dominant and recessive forms of the disease also exist • Parkinson disease is characterized by damage to the dopaminergic neurons Note; A complex interaction between environmental factors and genetic factors is implicated in pathogenesis of idiopathic Parkinson disease
Postulated theories • Oxidative injury may play a role • Neuromelanin , a product of dopamine aut oxidation is capable of forming a complex with iron and potentiates generation of free radicals and oxidative injury 2. Missence mutations causing extra copies of α-synuclein (which is presynaptic neurotransmitter) favors intracellular aggregation and protofibril formation of this protein
- and dopamine reacts with it a process that slow the process of protofibrils to fibril conversion and the protofibrils are toxic to the neurons and this may explain dopaminergic selectivity of α-synuclein associated PD • Age related decrease in neuronal cell volume and reduced proteasome degradation of α-synuclein may result in an increased intracellular accumulation of synucleinprotofibrils • Also aggregated α-synuclein binds to proteosomes and induces its dysfunction
Neurochemistry of parkinson disease • Loss of cells from substantianigra pars compacta leads to reduced inhibitory dopaminergic input into the striatum • This in turn results in increase release of GABA from striatum to lateral globuspallidus and to decreased its GABA release from lateral globus to Subthalamic nucleus , therefore the subthalamic nucleus production of excitaroygluatamte increases to the medial globuspallidus and then
medial globuspallidus will increase its release of inhibitory GABA to the thalamus • GABA is inhibitory so it will lead to decrease glutamate from thalmic nuclei to the cortex and this leads to akinetic rigid syndrome of parkinson
Gross:Pallor of the substantianigra and locus ceruleus. Microscopic features include : 1. Loss of the pigmented, neurons in these regions associated with gliosis. 2. Lewy bodies - May be found in those neurons that remain and these are single or multiple, intracytoplasmic, eosinophilic, inclusions that often have a dense core surrounded by a pale halo
. - UltrastructurallyLewy bodies consist of fine filaments, densely packed in the core but loose at the rim, composed of α-synuclein and other proteins, including neurofilaments and ubiquitin Note; , immunohistochemical staining for α-synuclein highlights more subtle Lewy bodies in many regions outside of the substantianigra - These lesions appear first in the medulla and then in the pons, before involvement of the substantianigra.
Lewy bodies eventually appear in the cerebral cortex and subcortical areas, including the basal nucleus of Meynert and the amygdala. Clinical Features : - It manifests as a movement disorder in the absence of a toxic exposure or other known underlying etiology and progresses over 10 to 15 years eventually producing severe motor slowing to the point of near immobility • Death usually is the result of inter-current infection
, or trauma from frequent falls caused by postural instability. - Movement symptoms of PD initially respond to l-dihydroxyphenylalanine (l-DOPA), but this treatment does not slow disease progression. • Over time, l-DOPA becomes less effective and begins to cause problematic fluctuations in motor function - While the movement disorder associated with loss of the nigrostriataldopaminergic pathway is an
important feature of PD, it is clear that the disease has more extensive clinical and pathologic manifestations. - Dementia, typically with a mildly fluctuating course and hallucinations, emerges in many persons with PD and is attributable to involvement of the cerebral cortex. - When dementia arises within 1 year of the onset of motor symptoms, it is referred to Lewy body dementia (LBD). .
Myopathic conditions: - Associated with segmental necrosis and regeneration of individual muscle fibers Examples of myopathies I. Dystrophinopathies: Duchenne and Becker Muscular Dystrophy - Are the most common form of muscular dystrophy - Are linked to mutations in the dystrophin gene. - Duchenne muscular dystrophy has an incidence of about 1 per 3500 live male births and follows a fatal course.
DMD becomes clinically evident by the age of 5 years; • most patients are wheelchair-bound by the time they are teenagers • and dead of their disease by early adulthood. - The Becker type of muscular dystrophy is less common and much less severe
MORPHOLOGY : The alterations in DMD and BMD are similar except that the changes are milder in BMD a. The hallmarks are myofiber necrosis and regeneration. b. Variation in myofiber size and internally placed nuclei. c. Progressive replacement of muscle tissue by fibrosis and fat and this will result in calf muscle hypertrophy - Both DMD and BMD also affect cardiac muscles, which show myofiber hypertrophy and interstitial fibrosis.
PATHOGENESIS : Both DMD and BMD are caused by loss-of-function mutations in dystrophin gene located on X Ch. - Dystrophin is a very large protein (427 kD) found in skeletal and cardiac muscle, brain and peripheral nerves; - It is part of the dystrophin-glycoprotein complex, which stabilizes the muscle membranes cell during contraction and involved in cell signaling through interaction with other proteins.
- The complex defects are thought to make muscle cells vulnerable to transient membrane tears during contraction that lead to calcium influx resulting in degeneration of myofiber that with time out paces the capacity for repair. - The dystrophin-glycoprotein complex also is important for cardiac muscle function; this explains why cardiomyopathy eventually develops in many patients.
- Muscle biopsy from patients with DMD show a complete absence of dystrophin, whereas patients with BMD have mutations that permit some dystrophin (albeit often a defective form) to be made Clinical Features - Often the first symptoms of DMD is delay in motor milestones - The weakness typically begins in the pelvic girdle and next involves the shoulder girdle.
- And the weakness can be demonstrated by Gower sign, the patient is inable to stand up from the floor without stabilizing himself by his hands - Enlargement of the calf muscles, termed pseudohypertrophy, is an important early physical finding. - The increased muscle bulk initially stems from myofiber hypertrophy, but as myofibers progressively degenerate, an increasing part of the muscle is replaced by adipose tissue and endomysial fibrosis.
- Cardiac muscle damage lead to heart failure and arrhythmias, which may prove fatal. - Although no structural abnormalities in the central nervous system have been described, cognitive impairment is also sometimes seen and may be severe enough to manifest as mental retardation - Owing to ongoing muscle degeneration, high serum creatinekinase levels are present at birth and persist through the first decade of life but fall as muscle mass is lost during disease progression.
. - Loss of ambulation is at age of 16 in DMD and later in BMD - Death results from respiratory insufficiency, pneumonia, and cardiac decompensation. - BMD becomes symptomatic in childhood or adolescence and progresses at a slower and variable rate. - Many patients live well into adulthood and have a nearly normal life span. - Cardiac involvement can be the dominant clinical feature and may result in death in the absence of significant skeletal muscle weakness