Download
1 / 43
440 likes | 645 Views
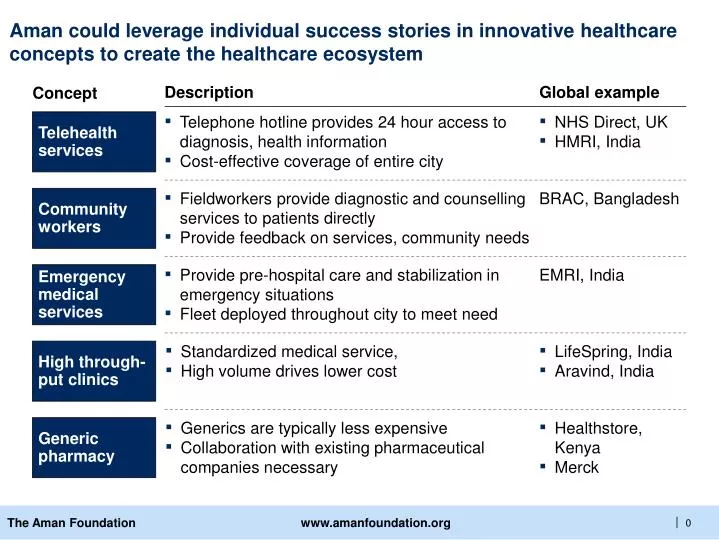
Telehealth services. Telephone hotline provides 24 hour access to diagnosis, health information Cost-effective coverage of entire city. NHS Direct, UK HMRI, India . Community workers. Fieldworkers provide diagnostic and counselling services to patients directly

E N D
Telehealth services • Telephone hotline provides 24 hour access to diagnosis, health information • Cost-effective coverage of entire city • NHS Direct, UK • HMRI, India Community workers • Fieldworkers provide diagnostic and counselling services to patients directly • Provide feedback on services, community needs BRAC, Bangladesh Emergencymedical services • Provide pre-hospital care and stabilization in emergency situations • Fleet deployed throughout city to meet need EMRI, India High through-put clinics • Standardized medical service, • High volume drives lower cost • LifeSpring, India • Aravind, India Generic pharmacy • Generics are typically less expensive • Collaboration with existing pharmaceutical companies necessary • Healthstore, Kenya • Merck Aman could leverage individual success stories in innovative healthcare concepts to create the healthcare ecosystem Description Global example Concept
Several organizations around the world offer health information hotline services via a central hotline and through other channels NHS Direct is the clear industry leader Focus of best-practice discussion U.K. Australia China South Africa India (AP) New Zealand 1 Based on monthly call volume: (calls per month/total population) * 1000 SOURCE: Company Web sites; customer interviews; employee interviews; press releases; press search
Key lessons from UK’s National Health Service Direct telehealth service NHS Learning Immediate relevance to Aman ü 1 NHS Direct’s 67% compound annual growth rate is achievable, even in a developed country with arguably reasonable health-care infrastructureA well-designed, interactive Web site can reduce strain on call centre and increase accessibility and convenienceUtilize technology and expand into new channels can increase reach and improve effectivenessAggressive marketing focused on key segments will help proliferate service Technology such as “profiling” can increase demand forecasting and improve customer relationships Necessary to provide home remedies whenever possible, rather than giving a doctor’s referral û 2 û 3 ü 4 ü 5 ü 6 SOURCE: Company Web sites; interviews; team analysis
2004-2005 Plans 2007 Piloted 1998 NHS Direct has utilized technology to increase and enhance service offerings with time Easier and faster advice and information about health, illness, and health services to enable clients to make decisions about their family’s health care Mission Indicates launch of new technology • Planning Podcast, videos, and online communities for Web site • Considering profiling technology to predict impact of a variety of external factors on customers to improve supply management and CRM • Linking Web site to call centre to allow online users to communicate with nurses using the Internet • All prior services • Appointment booking line • Relaunch of Web site to include mind and body magazine, new algorithms, improved accessibility (font sizes, languages) • Digital TV content development including increased number of health-information pages and new videos on various health- related issues • Voice over Internet protocol (VOIP) technology to match caller ID to patient records • 1998 services • Web site: comprehensive medical information (through interactive self-help guide [algorithms]), listing of NHS services (directory information), health encyclopaedia, articles on hot health topics • Digital TV: 24/7 access to information about ailments and treatments Description/ offerings • Cooperative GP service to handle out-of-hour calls • 24-hour, nurse-led telephone advice and information service funded by the government Number of contracts • Serviced 5.2 M calls in first three years • 500,000 calls/month • More than 1 M visitors to Web site/month • 500,000 digital TV viewers/month • 600,000 calls/month • 2.2 M visitors to Web site/month • Increased digital TV access to cover 68% of homes SOURCE: NHS Direct annual report; NHS Direct Web site; “NHS Direct: customer focus in the public sector,” case study, Imperial College, London, 2004
NHS Direct hotline service overview Call-center service offerings: • Free, 24-hour nurse-led telephone hotline providing: • Health advice and information based on symptom-based algorithms • Health directory of all medical facilities and pharmacies searchable by post code • Appointment booking service • Service offered in 40 different languages Call process: • Caller gives call taker personal details and is transferred to a nurse who uses algorithm-based questions to make a decision on the level of emergency and possible immediate home-care remedies (currently awaiting call transcription from NHS Direct) Call volume:Number of calls per year 67% 1999 2000 01 02 03 04 05 06 2007 SOURCE: NHS Direct annual report; Commission for Health Improvement sector report, 2004
5 NHS Direct’s web site offers a variety of information and services Web-site service offerings Language, font-size, and speech-tool options increase accessibilityProvides key word, body part, and subject search health encyclopaedia for information related to medical conditions, symptoms, health tests, treatments, operations, and servicesOffers answers to common health questionsOffers self-help guide that uses algorithm-based questions to determine severity of health concern – directing customers to adequate health-care channelIncludes articles relevant to the season/holidayOffers a health-service-information directory searchable by postal codeIncludes “Mind & body magazine” articles about preventive healthProvides clinical-enquiry services that allow people to send online questions to nurses who would reply (improves accessibility) SOURCE: NHS Direct Web site
Target audience:single men, aged 24-35 NHS Direct TV improves accessibility to health information, and it is available in 68% of U.K. homes NHS Direct TV service offerings Gives access to 3,000 pages of content through Freeview or Sky Digital on channel 108Provides answers to commonly asked health questions, hot topics hitting the headlines, and a guide to healthy livingOffers special features on diabetes, asthma, quitting smoking, STIs, diet, pregnancy exercises, and childhood illnessesShows extensive videos on topics including pregnancy and childbirth, healthy eating recipes, anger management, and sexual educationUse remote control to click through content including photos, illustrations, text, and video clips Service is also available in Urdu (Advertising campaign) SOURCE: NHS Direct Web site
2,000 HMRI’s virtual health-care delivery in India Overview Key challenges Description • Not-for-profit Institute, providing multiple health services through call centres • Provide large-scale virtual health-care delivery • Populations in Andhra Pradesh, India, who do not currently have access to proper medical care • Finding the right kind of management talent to build and manage the operations of the various services (e.g., TeleMedicine, TeleMonitoring) • Engaging the operational-level people (e.g., village health workers) to perform their jobs properly, including reporting back to monitor diseases in their regions • Preventing theft or loss of equipment (e.g., computers deployed in hospitals, mobile phones used by village health workers, ultrasound scanners in mobile units) • Educating families in rural areas (e.g., convincing in-laws to allow pregnant women to deliver in hospitals to reduce maternal mortality rate) • Maintaining high energy and high levels of services, long after the initial rollout is done (a typical challenge for publicly funded initiatives, whereby the quality of service deteriorates without good oversight) Objective Beneficiaries Contributions of key stakeholders • Private sector IT services company provides call centre technology and infrastructure • Government provides toll-free access • NGOs work on spreading awareness in the communities Private sector Public sector Social sector Scale Approach • Project is in very early stages but has major aspirations: • Aims to support 1.2 M people daily who currently don’t have access to proper medical care • Wants to help prevent 100,000 potential deaths each year • Plan to roll out to coverage area of 80 M people within first year • Provide a range of virtual services through call centre infrastructure including: • Telemonitoring (e.g., routine checkups during pregnancy or over period of child’s development) • Telemedicine • Tele-learning and public education SOURCE: HMRI, team analysis
Government • Government of India: toll- free access • State government Infrastructure HMRI Private sector • Not-for-profit Institute, mandated by Andhra Pradesh government to provide tele-distance health services across the state • Satyam Computers is providing funding and developing the software systems Social sector • NGOS that already have presence in communities to generate awareness of new service HMRI’s success hinges on the involvement of a broad set of players that came together with different motivations and assets
2,000 BRAC integrated health programs in Bangladesh Overview Key challenges Description NGO provides basic health services through 11 core programs focused on improving maternal, and child health, reducing vulnerability to common diseases, and controlling infectious diseases • Initial challenges in recruiting and training community-based volunteer health workers (“Shastho Shebikas”) • Developing infrastructure and capabilities to deliver training programs at scale • Need to build leadership capacity within organization to deal with growing scale and complexity of the organization • Potentially hire external talent with relevant expertise • Continue to provide opportunities for existing staff to grow and develop • Future challenge in expanding to new geographies and defining overall strategic direction for the organization • Need to identify new capabilities required (e.g., language skills) • Need to focus on areas where BRAC can have distinctive impact Objective Reduce poverty by providing improved health care as well as education and microfinance Beneficiary Low-income population (initially focused in Bangladesh) Contributions of key stakeholders Packaged goods companies (e.g., Unilever) provide social marketing to promote healthful practices (e.g., washing hands) Private sector Public sector Government of Bangladesh partners in implementing national programs; Bilateral agencies (e.g., Dutch govt) provide funding Social sector BRAC implements programs, trains health volunteers and mobilizes community involvement; NGOs provide technical assistance and coordinate activities with BRAC Approach Scale • Community-based health-care delivery • Provided primarily by volunteers who visit neighbouring households to provide basic health services and products • BRAC employees lead monthly workshops and run clinics that provide additional services to community • Develop new pilots and scale them through extensive infrastructure (e.g., sanitation project) • Significant impact in Bangladesh since establishment in 1972: • Provides basic health services to 31 M people • Tuberculosis control program reaches 83 M people • 68,000 trained health volunteers • 37 health-care facilities • Aspiration to grow internationally (incl. 10 countries in Africa) SOURCE: BRAC Health Program Annual Report, interviews, team analysis
BRAC is successful because it focuses on involving a broad set of players that came together with different motivations and assets Tuberculosis Program, Bangladesh government NGO with strong presence in rural villages • National program to fight TB • Agreement with BRAC to share facilities and personnel to identify suspects for treatment 1 • Extensive reach/coverage • Access to ~30 M people • 60,000 health volunteers in the field 2 Strong community relationships WASH Program, Dutch government • National budget allocated to contributing to MDG1 in sanitation • Agreement with BRAC for five-year program to change the way communities behave toward hygiene and for construction of minimum sanitation facilities 3 • Organizational capacity to run large-scale programs • Training and capability building programs to reach all its networks • Strong monitoring and evaluation systems in place 1 Millennium Development Goals SOURCE: Team analysis; Interviews
Transforming communities requires empowering and involving them as the owners of change Example of community involvement: BRAC approach • Creation of village committees with those key leaders to engage them in promoting the new initiatives for women Engagement of village leaders • Group of ~20 women from the community starts a BRAC VO with the aim of improving their socioeconomic position • They have weekly meetings in which they cover different topics and initiatives (microfinance, education, health, legal rights, etc.) • They have a commitment and responsibility as • a group in bringing change to their families Creation of village organizations (VOs) • Health volunteers: Members of the VO that are elected by the group (sense of status) • They provide health education, sell essential health commodities, collect basic health information, and refer patients to health centres, earning money from selling essential health commodities Community-based volunteers to work on specific programs • For example, health services are almost 99% subsidized but patients must make a symbolic payment (insignificant quantity) or make a deposit until they get healthy Everyone has to “pay” to show his/her commitment
BRAC: integrated health programs in Bangladesh • Business description • Social impact • Organizational approach • Critical considerations for scale a b c d
Overall approach a BRAC uses a holistic, grassroots approach to development which has proved to be more effective than top-down models Traditional NGOs/bilateral organizations Activity BRAC • Focus on achieving long-term, sustainable impact • Maintain commitment to specific communities, often prioritized on basis of lack of coverage by other NGOs or severity of conditions • Focus on outcome-based targets (e.g., reach x million people in a given period) • Pick geographies based on availability of resources and political factors (e.g., high-profile regions) Program design & definition of objectives • Mobilize communities • Engage key individuals to get buy-in • Train community to understand objectives and contribute their own ideas/resources to bring change • Engage government in shaping policies and implementing programs at national scale • Ensure high level of transparency to donors and community (e.g., on cost structure, sources of income criteria for participation) • Treat community as beneficiaries rather than partners • Maintain primary responsibility for decision making and tight control of resources • Demonstrate limited willingness to deal with perceived bureaucracy, corruption, and complexity of government • Lack formal accountability to external stakeholders Program implementation SOURCE: Interviews, team analysis
80 Overall approach a BRAC also focuses on self-sufficiency, using market-based approaches to subsidize its non-revenue-generating activities Sources of revenues Sample expenses $330 M • Bilateral groups (e.g., Dutch government, the Global Fund) and other donors • Government of Bangladesh • Salaries for paid BRAC staff • Currently employs 26,000 full-time staff and 34,000 part-time staff • Pays salaries competitive with other NGOs • Training (of staff and community), e.g., • Costs $28 to provide initial training for each of the 68,000 health-care volunteers (Shastho Shebika) • Costs 50c for monthly refresher courses • Maintain 14 training centres to deliver this type of training • Infrastructure and operating costs, e.g., • Run 31 health centres and various treatment-specific facilities (e.g., birth centres, BRAC limb and brace centre) • Provide free supplies to patients (e.g., “birth kits”) Grants & donations 30% • Microfinance program (charges 12.5% interest) • BRAC Enterprises (includes agri-processing, printing press, and others) • Service-based revenues, e.g., health centres • Operate at 60% cost recovery • Free for members of target communities; charge higher-income patients direct cost of services Self- generated 70% 2006 SOURCE: BRAC Annual Health Program Report, BRAC Web site, interviews, team analysis
Health programs • Total population: 125 M • Tuberculosis program reaches 83 M • Essential health-care program reaches 33 M and operates across all 64 districts in Bangladesh a BRAC’S health programs have achieved national scale within Bangladesh SOURCE: BRAC Health Program Annual Report
Health programs 2 National Tuberculosis Program Water and Sanitation (WASH) Program Maternal and Child Health (MNCH) Program 1 Essential Health Care (EHC) Program • Established in 1991 • Delivers free basic health-care services through a network of mobile health workers • Involves women from the community who are participants in BRAC’s microfinance program • Reaches 33 M people a BRAC ‘cracked the code’ for working on community health through its EHC program, which it now uses as a foundation for delivering several other health programs SOURCE: BRAC Annual Health Program Report, interviews
Health programs Shastho Shebika (SS) Program Organizer (PO) Village Organization (VO) Shastho Kormi (SK) a1 Key players in BRAC essential health-care program Description Role • Volunteer health workers • Monitor 200 households (visit ~15 households each day); refer patients to clinics if needed • Recruited from groups of women participating in microfinance program • Sell drugs and health-related products • 68,000 trained (attend 15-day program, monthly refresher courses) • Host monthly village health forums and antenatal clinics with POs and Shastho Kormis • Paid BRAC staff (largely women) responsible for supervising SSs • Supervise and support 10 to 15 SSs • Required to be high school educated • Host monthly village health forums and antenatal clinics • Attend 15-day training program • Paid BRAC staff responsible for directly supervising SKs • Supervise and support 6 or 8 SKs and 70 to 80 SSs • Typically recruit college graduates30 to 40 per region • Lead implementation of specific programs (EHC, tuberculosis, HIV/malaria) including collaboration with government and linkage with other BRAC activities • Households owning less than 0.5 decimals of land, lacking productive assets, and highly dependent on manual labour • Participate in BRAC microfinance, education, and health-care programs • 170,000 VOs formed • Provide feedback through randomized monitoring and evaluation surveys SOURCE: BRAC Annual Health Program Report, interviews
Health programs MNCH Tuberculosis control WASH a2 Stability of BRAC EHC model allows vertical programs to be integrated at various levels of the organization WORK IN PROGRESS Objectives Linkage to EHC program Impact/implications • Health volunteers • Refer people to clinic for testing • Provide drugs for patients undergoing treatment • Host health forums to educate community • Train health volunteers to recognize TB symptoms and effectively administer treatment • Reach 37 M people in 50 subdistricts by 2011 • Village organizations • Create committees to support program • Elect leaders to monitor progress • Build trust with community to influence them to invest in improving sanitation conditions • Achieve national goal of 100% sanitation by 2010 • Health workers • Run monthly antenatal health clinics • Train health workers to provide antenatal care • Improve maternal, neonatal, and child health status (and contribute to achieving MDGs 4 and 51) 1 Millennium Development Goal 4: reduce by 2/3 the mortality rate among children under five, Goal 5: reduce by 3/4 the maternal mortality ratio SOURCE: BRAC Annual Health Program Report, interviews
BRAC Grameen Members served (microfinance) 3.8 M 2.4 M Members served (health) 31 M 0 Members served (education) 1.1 M 0 Members trained 600,000 0 Number of villages covered 64,000 41.000 Number of employees 26,000 full-time 34,000 part-time 11,752 Annual loans disbursed ($ millions) 317 171 Average loan size $100 $110 % activities sponsored by donors 20% 0% Number of countries present in 2 24 (through network) Income generated by commercial activities (taka million) 2,881 150 (est.) b BRAC is one of the largest NGOs in the world and its direct impact exceeds that of prominent organizations such as Grameen bank Note: These figures represent activities in 2005 SOURCE: BRAC and Grameen Web sites
Community b BRAC currently leverages its approach to effectively develop partnerships with the government, bilateral donors and other organizations, and expand its impact Brac’s strengths Local government 1 • Extensive reach/coverage • Access to ~80 M people • 60,000 health volunteers on the field • Agreement to run TB program 2 • Community relationships • Model of empowerment of village women by bringing new roles to them (e.g., health worker) • Model of influencing community behaviours through creation of village committees International aid • WASH program funded by Dutch government • Organizational capacity to run large-scale programs • Organization of health workers, program organizers, paramedics that has the skills to roll out new programs • Training and capability-building programs that reach all of its network and to implement with other NGOs • Monitoring and evaluation systems in place 3 Private companies • Heath products distribution, e.g., Unilever
c BRAC has aligned its organization to work effectively with the community and developed capabilities to support its core programs 3 1 BRAC capabilities/infrastructure BRAC headquarters BRAC university BRAC enterprises Education Health care Microfinance BRAC training centres BRAC clinics BRAC field operations Regional health coordinators 1 • BRAC staff operate under three core programs that all deliver impact to community through the village organizations Program officers and health supervisors 2 Community involvement reinforces behaviour changes and allows BRAC to extend reach beyond its own staff capacity 2 Community Village organizations 3 Capabilities and resources effectively support activities of staff and community (e.g., provide training, funding) Committee leaders Volunteer health workers SOURCE: BRAC Annual Health Program Report, interviews
Build leadership within organization Develop healthy partnerships Take successful pilots to scale d BRAC’s approach shows the importance of combining good people and good strategy to address challenges to scale BRAC approach Growth challenge PEOPLE • Hire externally to complement strong culture of in-house learning and apprenticeship • Leverage BRAC university and partnerships with other university to build capabilities (e.g., language training) • Develop stronger capabilities to deal with increased complexity and size of organization • Create new capabilities to facilitate expansion to new markets STRATEGY • Negotiate agreements with government that do not involve contractor/contractee relationships (i.e., get independent funding and define clear responsibilities) • Involve multiple private-sector partners instead of committing to exclusive arrangements with a single partner • Maintain autonomy and flexibility to consistently implement model (e.g., provide same level of interaction with community) • Focus on “efficiency and effectiveness” • Identify critical components of model (take away nonessential parts) • Standardize process and make efficient • Build staff and management capabilities • Create monitoring system • Roll out and allow for adaptations • Rapidly and effectively replicate programs that have proved impact SOURCE: Interviews, team analysis
d BRAC: performance against key considerations and challenges ahead Current status Challenges ahead Partnerships • Partner with community to implement and monitor programs (e.g., by forming committees or training women to provide services) • Work with government to implement national programs (e.g., tuberculosis treatment and screening) • Work with private sector to implement social marketing campaigns (e.g., promoting sanitation) • Explore ways to partner with companies or organizations to fill un-met needs or to transition certain initiatives from grant-based to market-based models (e.g., housing) • Delivers large-scale training programs for field-based workers • Provides both introductory and follow-up training • Established specific training centres • Created university to provide training in NGO leadership and management • Trains BRAC employees and broader populations • Increasing need for leadership development to deal with growing complexity of organization • Additional skills required to support expansion into new geographies (e.g., language training) Capability building • Decentralized structure that encourages autonomy and innovation • Strong learning culture • Must strike balance between hiring external talent and providing growth opportunities for people within the organization Organizational approach SOURCE: Team analysis
3.6 Compared with $35 per capita spent every year in India 1-800 Save a Life How much would it cost? Expenditure per capita per year, $ INDIA EXAMPLE • For 1 cent per head per day, rural populations in India could get: • Efficient delivery of life-saving drugs • Access to field workers who would educate and build awareness • Access to qualified doctors who would diagnose and treat common ailments Cost model does not include: • Cost of drugs • Cold chain Capex1 Distributionopex2 Medical opex3 Total 1 Capex includes mobile phone, motorcycle, and technology 2 Distribution opex includes salaries, airtime for FW cell phone, and overhead 3 Medical opex includes doctors’ salaries SOURCE: 1-800-Save-a-Life cost model
Basic module Scale up – Full Scale up – Pilot Target population ~ 100 MM Managers 235 FWs 1500 Doctors ~380 Capex ~$3 MM Opex x 12 months ~$19 MM Total expense ~$35 MM Manager 1 Target population ~ 5 MM Managers 12 Field workers (FW) 75 Doctors ~20 Capex ~$170K Opex x 12 months ~$1600K Total expense ~$ 1.8 MM FW 6 Families/ day 58 • Key utilization assumptions (minutes/per day) • FW time spent per family 5 • FW communication time with manager 60 • FW travel time ~130 • Key outputs • Number of FWs per manager ~6 • Families visited per day 58 • Total population covered* ~66K 1-800 Save a Life Modularity and connectivity make the model scalable 1 Assumes a repeat visit every 6 months and an average rural family size of 8 SOURCE: 1-800-Save-a-Life utilization model
2,000 Description • Not-for-profit Institute, mandated by the Andhra Pradesh government to provide emergency response services across the state, under public-private partnership Objective • Provide integrated service for medical, police, and fire emergencies Public sector • Government provides toll-free access to designated number (“108”) Social sector • Universities train attendants; NGOs work on spreading awareness in the communities EMRI (‘108’) emergency management infrastructure in India Overview Key challenges • Need to identify or develop adequate leadership (i.e., individuals with the passion and competence to implement the program) in multiple regions across the country • Need to maintain and develop partnerships with various stakeholders, in particular, the government, hospitals, training institutions Beneficiaries • Inhabitants of Andhra Pradesh, India Contributions of key stakeholders Private sector • Private sector IT services company provides call centre technology and infrastructure; private hospitals stabilize emergency patients at no charge; donations of ambulances Scale • Scale to date: • Covers ~80 M population in Andhra Pradesh • 500 ambulances deployed • MoUs with more than 1,350 hospitals • Response to more than 250,000 emergencies • More than 14,000 lives saved since inception Approach • Provide quick, low-cost response to emergencies • Call centre dispatch answers within two rings • Ambulance arrives within 15 minutes (in 90% of cases) • Provide pre-hospital treatment through trained Emergency Medical Technicians who deliver care in ambulances, supported by doctors in the call centre • Use tiered pricing model based on destination hospital requested (e.g., patients going to private hospitals pay more) SOURCE: EMRI, team analysis
High volume, low cost maternal and paediatric clinics in India are helping combat maternal mortality Case Study: A clinic that delivers on quality, not on cost • The Problem: The lack of access to affordable healthcare contributes to the high maternal mortality ratio in India. • The Prescription: An Acumen-funded network of Maternity and Child Healthcare hospitals that provide vital reproductive and paediatric healthcare to low and lower-middle income people in urban and peri-urban areas, with a focus on delivering high quality, low-cost services to women and children in slum areas. The small hospitals (20-25 beds) are able to cater to a capacity of nearly 10,000 low-income patients every year • Achieving impact: The rates charged by LifeSpring Hospitals for general ward patients are less than one-third the market rate for normal deliveries and half the rate for caesarean deliveries; outpatient services are expected to cover over a million people over five years. • Applying the model: LifeSpring plans to use a franchising model to expand its coverage and could potentially export their model to Karachi. SOURCE: LifeSpring website, Acumen Fund website
High volume, low cost cataract surgery in India helps the blind see again Case Study: Restoring eyesight in India- a high volume approach • The Problem: India is home to about 20% of the world’s blind. Many of them suffer from treatable blindness due to cataracts but cannot afford the costly surgery to have their sight restored. • The Prescription: Inspired by McDonald’s low-cost production model, Aravind Eye Care System provides standardized cataract surgery and comprehensive ophthalmic care through hospitals, clinics, research facilities, and eye camp throughout India. By streamlining the surgical process, utilizing trained volunteers, and focusing on well-managed systems, Aravind accounts for 5% of India’s ophthalmic surgeries with only 1% of ophthalmic manpower. This ophthalmic network, the world’s largest, is also financially self-sustaining through cross-subsidization. Aravind was also awarded the 2008 Gates Award for Global Health. • Achieving impact: 2.3 million outpatient visits were handled and 270,444 surgeries were performed at the Aravind Eye Hospitals in 2006. Two-third of the outpatient visits and three-fourth of the surgeries were free of cost. • Applying the model: Aravind trains eye care professionals in its techniques and also provides support to hospitals interested in applying its management principles. Aman could work jointly with Layton Rahmatullah Benevolent Trust, establishing a link with Aravind and provide ophthalmic services in the clinic centre. SOURCE: Gates Foundation website, Aravind website
Child and Family Wellness (CFW) shops1 in Kenya deliveraffordable health care through franchises Overview Challenges Description Use of microbusiness franchise model to improve access to essential drugs and services • Current constraints to growth include: • Shortage of nurses with adequate business skills, experience, and commitment to run franchises (despite national shortage) • Performance of stores (financially and operationally) • Need to streamline organizational structure of the central office to effectively support field operations • The model has evolved since its inception to more effectively address some of the early challenges: • Revised selection criteria for franchise owners and locations to increase profitability • Improved quality and length of training programs for franchise owners Objective Lower cost of drugs and services and expand distribution networks Beneficiary Low-income population, Kenya Contributions of key stakeholders Private sector Franchise owners purchase drugs Public sector Regulations allow for franchises to exist The HealthStore Foundation provides technical assistance and ensures quality of franchise locations Social sector Approach Scale • Establish network of clinics and pharmacies • Owned by community health workers and licensed nurses who are able to supplement their incomes through these businesses • Ensure quality of products and services • Sell government-approved drugs • Conduct random spot-inspections on franchises • Leverage economies of scale • Lower drug costs through collective bargaining and bulk buying at wholesale prices • Centrally manage advertising and risk management • Progress since being founded in 2000 • 64 financially self-sustaining franchise locations • 750,000 patients served to date • Serves more than 400,000 patients per year in Kenya • Have temporarily suspended store growth to focus on improving in-store performance • Considering expanding range of product and services offered in existing stores (e.g., lab services, formal credit system) 1 Run by Healthstore Foundation formerly known as Sustainable Healthcare Enterprise Foundation (SHEF) SOURCE: Next Billion net, Columbia Business School case, team analysis
GAIN – Global Alliance for Improved Nutrition Organization profile Financial model & global partners • An alliance of governments, international organizations, the private sector and civil society. • Headquarters: Geneva, Switzerland. • Started: 2002 by Bill Gates and Kofi Anan • Objective: • Battling malnutrition by fortification of food • Focus on micronutrient deficiencies prevalent in vulnerable groups among the targeted countries • Helping the 190 UN-member states achieve the time-bound Millennium Development Goals of ending micro-nutrient deficiencies e.g. iodine, vitamin A, iron • Independent not-for-profit organization under Swiss law • Donors include: • Bill & Melinda Gates Foundation • Canadian International Development Agency (CIDA) • USAID • GAIN enjoys distinguished partnerships with: • Danone • Hellen Keller Intl. • Micronutrient initiative • World Food Programme • Tetra Pak • Unicef • Unilever • World Bank Institute Key strengths Board of Directors • Chunming Chen • Jamie Cooper-Hohn • Frances Davidson • Christopher Elias • Pierre Henchoz • Saad Houry • Richard Hurrell • Kai Kawabata • Olivier Kaiser • Ernest Loevinsohn • Jayaseelan Naidoo (Chairperson) • Dora Nkem Akunyili • Anji Reddy • Franck Riboud • Julian Schweitzer • Jamie Sepulveda • Paulus Verschuren • Bringing in all the relevant stakeholders under one entity, with one clear goal: fighting malnutrition • Forming national/regional business alliances, to deliver high quality, affordable nutrition to the most-in- need • Handing out grants to the best submitted proposals that are relevant to the organization’s mission and objectives • Leveraging its vast legacy of field experience, and wide communication network to replicate its model efficiently & effectively around the world • Constant monitoring and performance measurement to ensure continuous commitment towards agreed goals SOURCE: GAIN website
= GAIN regional offices • Francophone West Africa • Action: GAIN supported the Economic and Monetary Union of West Africa to organize a public-private dialogue on oil fortification • Impact: In March 2007, the Union and other partners united to promote the mandatory fortification of cooking oil with vitamin A for at least 70% of the population by 2010. • India • Action: GAIN initiated a food fortification project in the state of Gujarat. • Impact: the initiative reaches 400,000 nutrient deficient children aged between six and 36 months, now scaled up to reach 1 mil children Ghana • Action: Introduction of mandatory flour fortification, vegetable oil fortification, and upgrades quality control in the public and private sector. • Impact: Such initiative covers 80% of population, of which 4.4 mil are most vulnerable to anaemia. GAIN supports 19 projects in 18 countries, aiming to reach 1 billion people around the world • Georgia • Action: GAIN supports the Georgian National Fortification Alliance and Georgian NGO ACTS. • Impact: 280,000 metric tons of fortified wheat flour ,benefiting some 2.3 mil consumers. China • Action: GAIN has been working on a nation-wide policy for wheat fortification, and finally got approved by National Standards Standing Committee. • Impact: Iron-fortified soy sauce now reaches an estimated 33 million people at risk of iron deficiency SOURCE: GAIN 06-07 annual report
In 2005, The state of Nasarawa, Nigeria and Tetra Pak Food for Development (West Africa) Ltd. Have signed an agreement to distribute the fortified drink, ‘Nutri-Sip’ • In addition, the company also provides technical advice to the program, assisting in the development of management structures, addressing logistical challenges and helping to raise awareness about the program in communities • GAIN is assisting the Nasarawa government and Tetra Pak (West Africa) Ltd. by conducting an efficacy study of Nutri-Sip among Nigerian primary school children, in partnership with Helen Keller International (HKI) and Cornell University • The GAIN Business Alliance is the only global network dedicated to finding market-based business solutions to address the critical issue of malnutrition worldwide • The Alliance provides a forum where companies come together to develop new and innovative products, scale up existing fortification programs and identify new markets at national, regional or international levels • The ultimate goal of the alliance is to achieve a triple bottom line – increased profitability, public health benefits and local economic development and sustainability • In 2006, Grameen Danone Foods was established to provide healthy nutritious food accessible on a daily basis to people in Bangladesh with low incomes and vitamin and mineral deficiencies • In addition, Grameen Danone Foods will provide job opportunities in the farming, processing, sales and distribution sectors, with special emphasis on micro-financing and professional training to locals • GAIN is designing and rolling out a social marketing campaign for the yogurt and conducting an efficacy study in collaboration with John Hopkins University GAIN Business Alliance: Concept and examples of successful partnerships SOURCE: GAIN, web search
GAIN snapshots: the people, the process & the products SOURCE: GAIN, website
Edhi Foundation is planning similar large clinics and community centres Current services: High Ways Project ( 25 KILOMETRE) Under this project, it is planned to construct five hundred Edhi Centres in order to cover a sizeable population on all highways and major link-roads of Pakistan in a properly phased fashion. The existing centres provide first aid to accident victims and arrange for their speedy transfer to the nearby hospitals. More-over, these centres are being used for providing medical facilities in rural and semi-urban areas. Also they provide ambulance service at nominal charges, facility for vaccinating new-born babies and children against diseases, and other welfare services. The dispensary and mobile dispensary at each centre cater for medical assistance to approximately two hundred and fifty patients daily. On completion of the proposed project each Centre will have three ambulances, a four-bedded emergency unit, a permanent dispensary and a mobile dispensary for field operations. All Centres will be linked with wireless sets. Each centre is estimated to cost Rs. One million giving a total project cost of Rs. Five hundred million. Work has started on this project and sixty permanent and one hundred and twenty five temporary centres have already started functioning. Prospective services: Edhi Community Centres In its next phase of development, Highway Centres, which are mainly located in rural areas, shall be converted into community centres to create awareness regarding literacy, health, sanitation, safe drinking-water and immunisation. The programme will also support the community for solving their problems on self-help basis. Small loans will be granted for poultry farming and cattle breeding through Edhi Community Centres. Establishment of Specialised Centres for Treatment For treatment of renal problems and poor cancer patients, the Foundation hopes to build specialised hospitals and surgical units in Pakistan. SOURCE: Edhi Foundation website