Download
1 / 23
1.97k likes | 9.68k Views
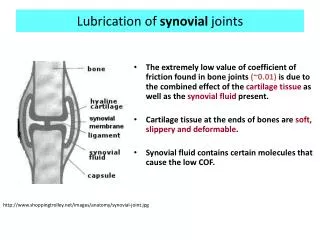
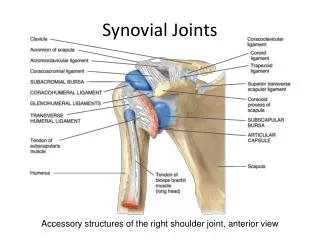
Synovial Fluid. I. Physiology & Composition Movable joints (diarthroses) composed of: Bones lined with articular cartilage Separated by a cavity containing synovial fluid enclosed in a synovial membrane Synovial membrane synoviocytes: Phagocytic – synthesizes degradative enzymes

E N D
Synovial Fluid • I. Physiology & Composition • Movable joints (diarthroses) composed of: • Bones lined with articular cartilage • Separated by a cavity containing synovial fluid enclosed in a synovial membrane • Synovial membrane • synoviocytes: • Phagocytic – synthesizes degradative enzymes • Synthesizes hyaluronate • Connective tissue • Blood vessels, lymphatics & nerves • Fluid formation • Ultrafiltrate of plasma across synovial membrane • Non selective • Excludes proteins of high molecular weight • Synoviocytes • Secrete mucopolysaccharite which contains: • Hyaluronic acid • protein
Cartilage & fluid function: • Reduce friction between bones • Lubricates joints • Fluid provides nutrients to cartilage • Lessens shock of walking and jogging impact Synovial Fluid – Normal Values Volume <3.5 mL Color pale yellow Clarity clear Viscosity forms string 4-6 cm long Erythrocytes <2000 cells/uL Leukocytes <200 cells/uL Neutrophils <20% of diff. Lymphocytes <15 % of diff. Monocytes & macrophages 65% of diff. Crystals NONE Glucose <10 mg/dL (lower than blood glucose) Lactate <250 mg/dL Total protein <3 g/dL Uric acid = blood value
Collection: arthrocentesis – needle aspiration of synovial fluid • Volume: • Normal= 3.5 mL • Diseased / inflamed = up to 25 mL • Collect 2 tubes • Heparin tube : microbiology • Plain top: chemistry and immunology • EDTA (liquid) : hematology *Avoid all powdered anticoagulants – interfere with crystal analysis • Fluid verification • Mucin clot test- • Add fluid to dilute acetic acid turbidity (clot formation) due to hyaluronate • Metachromatic staining • Place fluid on filter paper + few drops of toluidine blue metachromatic staining
III. Physical Examination • Color: • Normal – clear, pale yellow • Red to brown: indicates trauma of procedure or disorder • Turbidity: associated with presence of WBCs • Milky: may indicate presence of crystals • Viscosity: • Measured at bedside by ability to form a string from tip of syringe • Normal: 4-6 cm • Ropes test (mucin clot test)– measurement of hyaluronate polymerization • Fluid forms a clot surrounded by clear fluid when added to acetic acid • Clot quality is reported: • Good = solid clot • Fair = soft clot • Poor = friable clot • Very poor = no clot • Test is of questionable precision and seldom used
IV. Microscopic Examination • Cell Count – WBCs • Method • Use Neubauer counting chamber • May pretreat viscous fluids with hyaluronidase & incubate at 37oC for 5 min. • Dilution with hypotonic saline is used to lyse any RBCs OR • Dilute with normal saline/methylene blue mixture to differentiate WBCs from RBCs • Normal = <200 / uL • Differential Count • Cytocentrifuge specimen and prepare typical blood smear • Normal: 60% monocytes, macrophages neutrophils: <20% lymphocytes: <15% (* values vary between texts) • Increased neutrophils – possible septic condition • Increased lymphocytes – indicate nonspetic inflammation
Other cell abnormalities: • Increased eosinophils – rheumatic fever, parasitic infections, metastatic carcinoma, post radiation therapy or arthrography • LE cells – patients with lupus erythematosus • Reiter cells – macrophages with ingested neutrophils • RA cells (ragocytes) – precipitated rheumatoid factor appearing as cytoplasmic granules in neutrophils • Hemosiderin granules – due to hemorrhagic process or cases of pigmented villonodular synovitis • Cartilaginous cells – observed in cases of osteoarthritis • Rice bodies – found in septic and rheumatoid arthritis and Tuberculosis • Fat droplets – indicate traumatic injury
Crystals • Crystal formation may be due to: • Metabolic disorders • Decreased renal excretion • Cartilage and bone degeneration • Medicinal injection (ex: corticosteroids) • Fluid is examined using the wet preparation technique • ASAP examination as pH and temperature affect observation • Ideally examined prior to WBC disintegration • Examine under both direct and compensated polarizing light • *may also be observed in Wright stain preparations • Under polarizing light (Direct polarization) • Birefringent substances appear as bright objects on a black background • Intensity varies between substances • Under compensated polarizing light • A red compensator plate is placed between the crystal and slide • Crystals aligned parallel to the compensator appear yellow (negative birefringence) • Crystals aligned perpendicular to the compensator appear blue (positive birefringence)
Monosodium Urate Crystals (MSU) • Indicate gouty arthritis due to: • Increased serum uric acid • Decreased renal excretion of uric acid • Impaired metabolism of nucleic acid • Exhibit negative birefringence • Intracellular (acute stages) & extracellular location • Polarized light – strongly birefringent • Compensated polarized light – yellow when parallel blue when perpendicular • Needle shaped • Calcium pyrophosphate (CCPD) • Indicates pseudogout due to: • Degenerative arthritis • Endocrine disorders with increased serum calcium • Calcification of cartilage • Exhibit positive birefringence • Seen intracellular- and extracellularly • Polarized light – weakly birefringent • Compensated polarized light – blue when parallel (yellow when perpendicular) • Blunt rods or rhombic shapes
Cholesterol • Nonspecific indications • Associated with chronic inflammation • Exhibit negative birefringence (compensated polarized light) • Usually seen extracellularly • Polarized light – strongly birefringence • Rhombic plates • Hydroxyapatite (HA) (Calcium phosphate) • Associated with calcific deposition conditions • May produce an acute inflammatory reaction • Intracellular • Not birefringent • Require an electron microscope to examine • Small, needle shaped • Corticosteroid • Associated with intra-articular injections; NO clinical significance • Primarily intracellular • Exhibit positive and negative birefringence • Can closely resemble MSU and CCPD • Flat, variable shaped plates
Calcium Oxalate • Following renal dialysis • Birefringent Artifacts: • Anticoagulant crystals (calcium oxalate, lithium heparin) • Starch granules • Prosthesis fragments • Collagen fibers • Fibrin • Dust particles
V. Chemistry Tests • Glucose • Done simultaneously with blood sample (prefer 8 hour fast) • Difference between blood and synovial glucose values is evaluated • Normal = < 10 mg/dL • Inflammatory conditions = > 25mg/dL • Sepsis = >40 mg/dL • Considered low if < ½ serum plasma glucose value • Should be run within 1 hour of collection • Draw in sodium fluoride – prevents glycolysis • Total protein • Not routinely performed • Normal = < 1/3 of serum value (~3g/dL) • Large molecule, not easily filtered by membrane • Increased protein • Changes in membrane permeability • Increased joint synthesis • Indicates an inflammatory process
Uric Acid • Alone, not diagnostic • May determine gout in conjunction with plasma uric acid, esp. when crystals are undetectable • Normal = serum level • Lactate • May differentiate between inflammatory and septic arthritis • Septic arthritis = >250 mg/dL • Gonococcal arthritis = normal to low levels • Production results from : • Increased demand for energy • Tissue hypoxia • Severe inflammatory conditions
VI. Microbiology Tests • Gram stain • Performed on all specimens • Most infections are bacterial: • Staphylococcus • Streptococcus • S. pyogenes • S. pneumoniae • Hemophilus • Neisseria gonorrhea • Fungal, viral and tubercular agents may also be observed • Culture • Routine culture • Enrichment medium (chocolate agar • Specialty media depending on clinician orders and indications
VII. Serologic Tests • Autoantibody detection (same as found in serum) • Rheumatoid arthritis (RA) • Lupus erythematosus (LE) • Antibody detection in patient’s serum • Borrelia burgdorferi • Causative agent of Lyme disease • Cause of arthritis
VIII. Joint disorder classification Group Classification Significance • Noninflammatory Degenerative joint disorders • Inflammatory Immunologic problems (RA, LE) Gout & pseudogout (crystal induced) • Septic Microbial infection • Hemorrhagic Traumatic injury Coagulation deficiency Note: * categories overlap * multiple conditions can occur simultaneously * disease stage can vary laboratory results *see text for details of associated abnormal laboratory findings