Download
1 / 41
410 likes | 428 Views
Learn how to work with high conflict domestic violence clients, understand the common issues they face, the characteristics of personality disorders, and how to navigate interventions effectively.

E N D
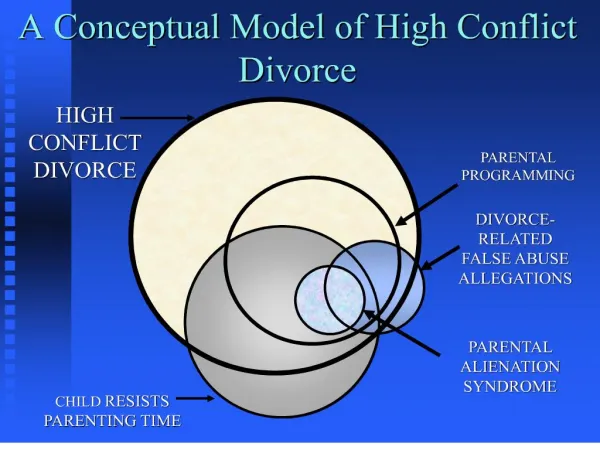
HIGH CONFLICT CLIENTS UNDERSTANDING & INTERVENING WITH HIGH CONFLICT DOMESTIC VIOLENCE CLIENTS Gary Gibbens, MaPsy
Reasons Not To Label People • Stigmatizes the client • Diagnosis may be incorrect • May affect counselor's view of and relationship with the client • Labeling without appropriate referral or change in treatment approach is not helpful
Common Issues of High Conflict Clients • Rigid and uncompromising • Difficulty accepting or processing loss • Can appear logical until emotions overwhelm logic • Avoids responsibility-focus on blaming • Depends on other people to solve problems • Limited ability to self reflect • Almost no empathy for other’s issues
The Paradox of High Conflict Clients The Paradigm shift for Intervention The HCC is always trying to focus on conflicts with others and trying to involve us in solving these conflicts The Real issue: Conflict is WITHIN these individuals
Characteristics of DSM-IV Personality Disorders • Enduring patterns of problem behavior from early childhood/adolescence • Extreme (all or nothing) thinking, emotions, behavior • Interpersonal dysfunction • Impulse control problems • Not the result of substance abuse or trauma
NIH Study 2001-02 National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism found: • 30.8 million Americans (14.8%) meet diagnostic criteria for at least one personality disorder under DSM-IV • These diagnoses were found to be highly associated with emotional disability and social dysfunction.
Maladaptive Personality Traits • Meet fewer DSM criteria than PD • Less rigid • Can function appropriately in some environments but exhibit dysfunctional traits in other environments (usually family, home) • Potentially more workable • Diagnosis not essential for intervention
Private Working Theory(William Eddy) Private: If you decide that you are working with a High Conflict Client, keep this information to yourself or share only with those you need to consult Working: Use your assessment to guide your approach to this client, not to judge or criticize Theory: Your assessment is only a theory and you may need to revise it as you work with the client
Levels of Conflict Functioning Non-disordered(“normal”) Client Appropriately upset about conflicts; able to resolve, de-escalate, and make adaptive changes. Maladaptive Personality Traits Appear “normal”, but show inappropriate upset; highly exaggerated ideation; distorted logic; ABLE to resolve conflicts with careful management. Personality Disorders Rigid pattern of behavior; chronic distress; chronic interpersonal dysfunction; tend to be unconscious of the effects of their own behavior; MAY not be able to resolve conflicts
Adapts to changing world as needed Able to accept feedback and change behavior Resilient & Flexible Conscious control of behavior Functions like a computer’s operating system Chronically fails to adapt to changing environment Repeats failed behavior, insists that others adapt to their viewpoint—self defeating Despite chronic, increasing consequences, does not adapt or change May have little conscious control Functions like a computer operating system that is constantly crashing Personalities Either:Adaptive or Maladaptive
Does not have Personality Disorder or Maladaptive Traits Can be self/aware Can turn high conflict behavior on and off Chooses: Not to Listen To Be Aggressive To Be Inflexible To Be Out of control Has Cluster B Personality Disorder or Traits: Borderline Narcissistic Antisocial Histrionic Despite Chronic Difficulties, does not adapt or change. May be unconscious of inappropriate social behavior Cluster C Personality Disorders Avoidant Dependent Obsessive-Compulsive High Conflict Clients: Styles vs. Traits/Personality
Negative Feedback Loop of High Conflict Clients • Chronic feelings of Distress • Views source of distress/problems as external • Fails to self reflect or self awareness distorted • Chronic feelings of being a victim • Feelings of Helplessness • Wants of relieve distress—may use alcohol/drugs at this point • Blames others (usually family), attempts to change others (often through abuse & violence), actively tries to recruit negative advocates. • Result is Negative feedback to Client—rejection, legal consequences, isolation—self defeating Behavior • Leads to chronic feelings of distress
Consequences of Negative Feedback Loop • HCC has long history of Negative Feedback • Experiences Feedback as a Threat • Rather than learning from Feedback, Defends against it (the four horsemen) • As Intensity of Feedback increases, Client defensiveness increases leading to abusive behavior—again may abuse substances • Result is more Internal Distress • Client repeats the Loop again
Motivated by: Perceived threats Defending self against losses Need to control or change others Narcissistic Injury Any change in system Pregnancy of victim Job change Illness, Injury HCC feels justified in acts of: Verbal, emotional abuse Physical abuse Stalking Legal abuse Self destructive behavior, suicide, cutting Sexual affairs Substance abuse HCC: Extremes Of Behavior
HCC: Extremes of Emotion • Explosive intense anger, panic, sadness, anxiety • When rational thought fails, they feel overwhelmed by emotions • Emotional outbursts get more attention, are more instrumental • Emotions help HCC generate facts to fit the emotion (distorted, paranoid) • Emotions supersede logic and problem-solving
Problems seen as overwhelming, unsolvable Sees self as victim Sees others as very powerful: either threatening enemies or life-saving allies Life-long development of high intensity bonding skills: charm, seductiveness, child-like appeal, emotional urgency, manipulation of reality, trauma bonding Results in “Instant Intimacy” Over responds to any emotional interactions Lack of boundaries Unrealistic infantile expectations lead to infantile emotional reactions HCC assumes no responsibility for maintaining relationship, solving problems Loss of relationship results in desperate attempts to re-attach, YO-YO behavior, attach to negative advocates HCC: Extremes of Dependency
Counsellors feel frustrated or frightened by their emotional sensitivity, abusive behavior, and dependency needs Counsellors get emotionally “hooked” and either withhold responses or over respond. William Eddy Use your EAR EMPATHY ATTENTION RESPECT Typical Responses to HCC
Negative Advocates • Believe cognitive distortions of HCC • Want to help • Misled or seduced by HCC’s charm, hurt, fear, anger, pain • Advocate against perceived enemies • Protect HCC from natural consequences • Escalate conflicts unintentionally • May also be HCC’s
Be a Positive Advocate • Avoid assumptions • Investigate concerns/problems • Provide support and information • Establish appropriate boundaries, avoid taking too much responsibility for problems and emotions • Avoid doing MORE work than HCC • Don’t rescue—HCC needs to feel natural consequences—but don’t automatically reject.
Developmental Basis for HCC: Paul MacLean’s Triune Brain "three interconnected biological computers, each with its own special intelligence, its own subjectivity, its own sense of time and space and its own memory". Each brain operates as its own brain system with distinct capacities for perceiving and responding to the environment and each can become dominant depending on the circumstances.
Three Levels of Brain Functioning Neocortex Cerebral Cortex or Cerebrum Center of abstract thought, creative thinking, all higher cognitive functions. Limbic System Middle part of brain, “old mammalian” concerned with emotions, instincts, feeding, fighting, fleeing, value judgements, sexual behaviour. Reptilian Brain Basal brain consists brain stem and cerebellum. Center of rigid, obsessive, compulsive, paranoid ideas and behaviour, never learning from past mistakes. Automatic functions; breathing, reflex, etc.
Left Hemisphere Logical Sequential Rational Analytical Objective Looks at parts Positive emotions Higher dopamine Right Hemisphere Random Intuitive Holistic Synthesizing Subjective Looks at wholes Negative emotions Higher norepinephrine Cerebral Cortex: 2 Hemispheres
Corpus Collosum • The corpus callosum is a bundle of nerve fibers that connects the two hemispheres of the brain, enabling them to work together to process information and regulate autonomic function • Area where the two hemispheres are “stitched” together—through nerve fibers • Left Brain needs input from the right, to process non-verbal information & process negative emotional input • Right needs input from the left to analyze information, to assess danger, to communicate verbally, to achieve positive emotions
Emotional Dysregulation of HCCs • Research with BPD and ASPD indicate brain differences in the Hippicampus and Corpus Collosum Working Theory HCCs have difficulty mediating powerful emotions with logic and rationality; as a result they are unable to self soothe or regain a sense of calm.
Flight or Fight Response • Under conditions of emotional or physical stress, the limbic system floods emergency systems with adrenaline to energize for quick reactions, over-riding the functions of the cerebral cortex. • Children who have been abused over-respond to “normal” situations and show developmental brain differences • HCCs tend to be HOT responders in handling stressful situations exhibiting distorted thinking about the situation
Cognitive Distortions • All or Nothing thinking • Magnification or Minimization • Should statements • Overgeneralizations • Jumping to conclusions • Personalization • Emotional reasoning
Intervention with Agitated HCCs • Help client shift focus to more Left Brain or integrated activities: Brain gym, breathing exercise, making a list of options and asking client to logically review choices, make lists, etc. • The shift to more “Left Brain” activities does not require solution of the conflict or problem. Client usually feels relief when you help them do this
Preparing Staff for HCCs • Emotional Grounding and self-care • Brain Gym • Good stress management skills • Maintaining clear Boundaries • Understand and Explore Counter-transference • Co-therapy groups if possible • Debriefing support • Avoid the extremes: Seduction by or rejection of the HCC • Avoid Trauma triggers
Service Agreements & Interventions • Program involvement—clear simple rules • Sobriety • Non-abusive Behaviour and Language • Client acceptance that problem behaviour has occurred • Acknowledges need for help • Accountable for own behaviour • Considerate & Aware of others • Involved in the process of Service Delivery • Avoids blaming others or systems
Karpman Triangle Persecutor Rescuer If you are vulnerable in any of these roles, a skilled HCC will find out and exploit it. Victim
Parent: Ingrained voice of authority. Value statements, Right or Wrong. Adult: Our 'Adult' is our ability to think and determine action for ourselves, based on received data. Child: This is the seeing, hearing, feeling, and emotional body of data within each of us. Transactional Analysis Parent Adult Child
Counselling with HCC • Listening with Neutral attention/respect to high intensity emotions (set time limits--avoid being bullied or rejecting client) • Focus on Tasks—structure sessions • Provide Active Reality Testing • Use low-level but clear Confrontations • Block development of Negative Advocates--Bullying • Reflect back their Self Talk process/point out inconsistencies • Incorporate Time Outs in group/individual tx process • Identify/emphasize Strengths • Help client learn to identify body stress or stressful emotions and “turn down the volume”
Listening to High-Intensity Emotions • HCCs attempt to establish relationships through trauma bonding. • They want to establish an unconditional “caring” relationship which they can control & exploit • Staff needs to be very aware of their own limits around emotional intensity • Staff needs to help HCCs shut down when the intensity becomes repetitive, obsessive, overwhelming to the client (Watch for looping, fight or flight arousal) Breathing, safe place exercises
Focus on Tasks • Whenever possible, move away from emotional expression and help client develop a “structure” for problem solving Example: Brain Gym, relaxation, writing down problems, brainstorming solutions • Help client break large overwhelming issues into small steps • If client agrees to tasks, always follow through to see if he/she has completed them
Provide Low-Level Confrontations • Be aware of HCC Over-reaction to any judgements, rejection, humiliation, abandonment • Statements like, “I wonder what else happened”– “It seems like you left something out”– “It just doesn’t make sense to me—I guess I don’t understand you” • Sometimes clear, low intensity value statements can be more effective than anything else • Don’t attack the relationship but Insist on Accountability • Hypotheticals can also work
Reflect Self Talk Process • Help client reconstruct linkage between stimulating event, self talk, emotional response and behaviour • Explore choices at every step in the linkage and involve client in feedback/problem solving. • Remember the PROBLEM(S) is almost always internal or inside the client’s mind & body
Listening to High Intensity Emotions • Model listening with respect & interest • Respond with caring, understanding statements if indicated • Avoid taking on their emotions/insist on client accountability • Be clear that staff cannot “fix” the problem • If conflict involves others, ask HCC to listen and respect feedback without interruption
Identify/Emphasize Strengths • HCC may have some part of life where they function non-abusively. (work, school, church) Help them identify area and what works for them in that part of their lives. • Work on developing new strengths in the program: Listening, Being aware of other’s needs, Taking responsibility, Taking Time Outs
Bibliography • Eddy, B. HIGH CONFLICT PEOPLE IN LEGAL DISPUTES, 2006 • Linehan, M. COGNITIVE-BEHAVIOUR TREATMENT OF BORDERLINE PERSONALITY DISORDER, 1993