Download
1 / 44
440 likes | 558 Views
1-C: Renal and Hepatic Elimination. 400 mg of moxifloxacin is administered orally to Mr BB, a 68 yr old male who weighs 75 kg. Blood samples were drawn following the dose and the plasma concentration determined. It is known that about 20% of a moxifloxacin dose is excreted in the

E N D
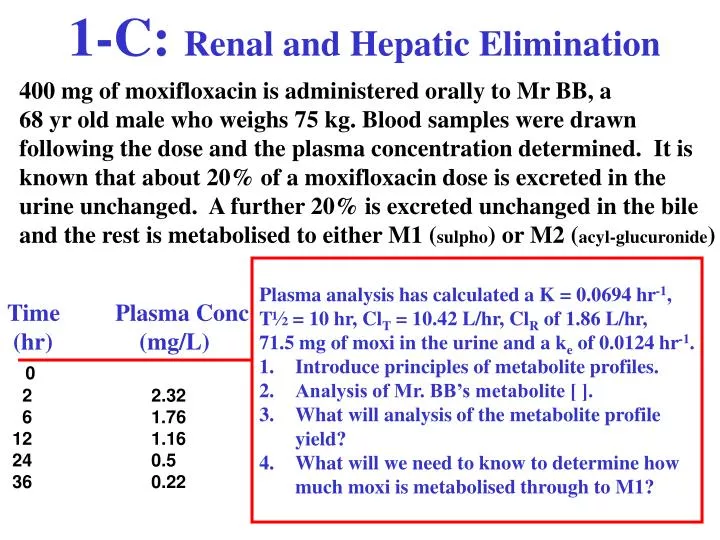
1-C: Renal and Hepatic Elimination 400 mg of moxifloxacin is administered orally to Mr BB, a 68 yr old male who weighs 75 kg. Blood samples were drawn following the dose and the plasma concentration determined. It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) • Plasma analysis has calculated a K = 0.0694 hr-1, • T½ = 10 hr, ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine and a ke of 0.0124 hr-1. • Introduce principles of metabolite profiles. • Analysis of Mr. BB’s metabolite [ ]. • What will analysis of the metabolite profile • yield? • What will we need to know to determine how • much moxi is metabolised through to M1? Time Plasma Conc (hr) (mg/L) 0 22.32 61.76 121.16 240.5 360.22
1-C: Renal and Hepatic Elimination 400 mg of moxifloxacin is administered orally to Mr BB, a 68 yr old male who weighs 75 kg. Blood samples were drawn following the dose and the plasma concentration determined. It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) • Plasma analysis has calculated a K = 0.0694 hr-1, • T½ = 10 hr, ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine and a ke of 0.0124 hr-1. • Introduce principles of metabolite profiles. • Analysis of Mr. BB’s metabolite [ ]. • What will analysis of the metabolite profile • yield? • What will we need to know to determine how • much moxi is metabolised through to M1? K = ke + kH + kNR ClT = ClR + ClH + ClNR
Models Describing Moxi Elimination It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) K = ke + kH + kNR ClT = ClR + ClH + ClNR K = ke + km1 + km2 + kNR ClT = ClR + Clm1 + Clm2 + ClNR
Models Describing Moxi Elimination It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) Focus on one metabolite (M1) which is reported to account for ~40 - 45% of moxifloxacin clearance. Although only 5-6% of the dose appears in the urine as M1 and the balance appears in feces as M1, for our purpose we will assume complete excretion of M1 into the urine. ~15% of the dose is metabolised through M2. The metabolite concentration in the body is a function of the rates of formation (km) and metabolite elimination (kme)
Models Describing Moxi Elimination It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) The metabolite concentration in the body is a function of the rates of formation (km) and metabolite elimination (kme) dM dt = km Dose - kmeM Which can be solved to produce this equation kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Which describes the concentration of metabolite following IV bolus administration of parent.
Models Describing Moxi Elimination It is known that about 20% of a moxifloxacin dose is excreted in the urine unchanged. A further 20% is excreted unchanged in the bile and the rest is metabolised to either M1 (sulpho) or M2 (acyl-glucuronide) There are a number of parameters in this equation which will require some calculation &/or may be difficult to estimate. kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) VM volume of metabolite, kme and km
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. Which one of kme or K will appear in the terminal phase? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Which one kme or K will be the smallest … or slowest?
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) In this profile which one is the smallest … or slowest? kme or K?
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Which one is the smallest … or slowest? kme or K? Here, since the parent compound’s profile following IV bolus administration has a faster half-life, kme appears to rate-limit elimination of the metabolite. K > kme and kme is rate limiting
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. Which one will be the smallest … or slowest? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) K = 0.08 K > kme 0.08 > 0.04 0.04
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Which one is the smallest … or slowest? kme or K? Here, since the parent compound’s profile following IV bolus administration has a faster half-life, kme appears to rate-limit elimination of the metabolite. Method of residuals should generate K from the metabolite profile
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. What happens when the metabolite, a very polar glucuronide, is excreted rapidly into the urine? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) )
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. What happens when the metabolite, a very polar glucuronide, is excreted rapidly into the urine? Now, kme >> K, & at some time (e–kmet) will approach zero and the equation will be effectively reduced to: kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) kmDose VM(K-kme) CM (e(-Kt))
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. What happens when the metabolite, a very polar glucuronide, is excreted rapidly into the urine? Now, kme >> K, then at some time (e–kmet) will approach zero and the equation will be effectively reduced to: kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Showing that at later times, the metabolite concentration-time profile will be parallel to the parent [ ]-time profile.
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Now, which one is the smallest … or slowest? kme or K? K = 0.08 Kme > K = 0.2
The case of the Rate-Limiting Exponential The CM equation is very similar to the bi-exponential oral equation. The two exponentials are now Kme and K. Which one is the smallest … or slowest? kme or K? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Here, since the parent compound’s profile following IV bolus administration has a half-life equal to metabolite, K appears to rate-limit elimination of the metabolite. Method of residuals should generate kme from the metabolite profile
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) )
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Since K = ke + km Then as km approaches K, less drug could be excreted unchanged and ke would approach zero. ClR ke ke Ae0- ClT K k10 DoseIV ----- = ----- = ----- = ---------
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Since K = ke + km Then as km approaches K, less drug could be excreted unchanged and ke would approach zero. ClR ke ke Ae0- ClT K k10 DoseIV ----- = ----- = ----- = --------- km/K represents the fraction metabolised just as ke/K represents the amount excreted unchanged into the urine
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 and km = 0.02 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • 2. What fraction of the dose is metabolised?
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 and km = 0.02 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • K • What fraction of the dose is metabolised? K = 0.08 0.02 0.20
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 and km = 0.02 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • K • What fraction of the dose is metabolised? • km/K = 0.02/0.08 = 25%
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 but km is increased to = 0.07 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • What fraction of the dose is metabolised? K = 0.08 0.02 0.20
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 but km is increased to = 0.07 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • K • What fraction of the dose is metabolised? K = 0.08 0.02 0.20
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? kmDose VM(K-kme) CM = (e(-kmet) - e(-Kt) ) Consider the situation where K = 0.08 hr-1, kme = 0.2 hr-1 but km is increased to = 0.07 hr-1. • Questions: • The metabolite profile is rate limited by which exponential? • K • What fraction of the dose is metabolised? • km/K = 0.07/0.08 = 87.5%
The effect of km on the metabolite profile km is not one of the exponentials in a metabolite profile So, how does km affect the metabolite profile? km/K = 0.02 / 0.08 = 25% km/K = 0.07 / 0.08 = 87.5% Peak = 0.621 mg/L Peak = 0.177 mg/L
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Parent M1 Time Plasma Conc. Plasma Conc (hr) (mg/L) (mg/L) 0 1 2.49 0.18 22.32 0.31 3 2.17 0.41 4 2.02 0.48 61.76 0.56 8 1.53 0.58 121.16 0.53 240.5 0.28 360.22 0.13 • Plasma analysis has calculated a • K = 0.0694 hr-1, T½ = 10 hr, • ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine • and a ke of 0.0124 hr-1. • Introduce principles of • metabolite profiles. • 2. Analysis of metabolite [ ]. • What will analysis of the • metabolite profile yield? • What will we need to know • to determine how much moxi • is metabolised through to M1?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Parent M1 Time Plasma Conc. Plasma Conc (hr) (mg/L) (mg/L) 0 1 2.49 0.18 22.32 0.31 3 2.17 0.41 4 2.02 0.48 61.76 0.56 8 1.53 0.58 121.16 0.53 240.5 0.28 360.22 0.13 • Plasma analysis has calculated a • K = 0.0694 hr-1, T½ = 10 hr, • ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine • and a ke of 0.0124 hr-1. • Introduce principles of • metabolite profiles. • 2. Analysis of metabolite [ ]. • 3. What will analysis of the • metabolite profile yield? • What will we need to know • to determine how much moxi • is metabolised through to M1?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? • Plasma analysis has calculated a • K = 0.0694 hr-1, T½ = 10 hr, • ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine • and a ke of 0.0124 hr-1. • Introduce principles of • metabolite profiles. • 2. Analysis of metabolite [ ]. • What will analysis of the • metabolite profile yield? • What will we need to know • to determine how much moxi • is metabolised through to M1?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Slope of the terminal phase is likely to yield a value for which exponential ??…
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Slope of the terminal phase is likely to yield a value for which exponential ??… Metabolite profile is parallel to the elimination of the parent compound… therefore, the terminal phase is likely to yield a value for K.
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Slope of the terminal phase is likely to yield a value for which exponential ??… K And the method of residuals from plasma metabolite data will like yield a value for what exponential?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? Slope of the terminal phase is likely to yield a value for which exponential ??… K And the method of residuals from plasma metabolite data will like yield a value for what exponential? kme
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? • Plasma analysis has calculated a • K = 0.0694 hr-1, T½ = 10 hr, • ClT = 10.42 L/hr, ClR of 1.86 L/hr, • 71.5 mg of moxi in the urine • and a ke of 0.0124 hr-1. • Introduce principles of • metabolite profiles. • 2. Analysis of metabolite [ ]. • 3. What will analysis of the • metabolite profile yield? • 4. What will we need to know • to determine how much moxi • is metabolised through to M1?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? What will we need to know to determine how much Moxi is metabolised through to M1?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? What will we need to know to determine how much Moxi is metabolised through to M1? Since we made the assumption that all M1 was excreted into the urine, the amount of metabolite found in the urine (Ame0-∞) Ame0-∞ km DoseIV K ------------ = -------
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? What would we observe if we had a pure sample of M1 and we administered it IV?
1-C: Renal and Hepatic Elimination Following a 400 mg of moxifloxacin to Mr BB, the following concentrations of parent and metabolite are observed. It is known that about ~18% of the moxi dose in this patient is excreted into the urine unchanged. How much is metabolised through to M1? What would we observe if we had a pure sample of M1 and we administered it IV? Elimination rate would be kme, and the value would be the same as if we had completed the method of residuals on the metabolite profile.
1-C: Renal and Hepatic Elimination Metabolite Summary Metabolites are chemically distinct and differ from the parent compound. A metabolite will have its own : Distribution space Clearance “Fate” Compartmental Model [ ]vs. time profile A metabolite can be excreted into the urine or bile directly or further metabolised. Metabolite
1-C: Renal and Hepatic Elimination Since K = ke + km1 + km2 + kNR and ClT = ClR + Clm1 + Clm2 + ClNR and the clearance of individual processes can be calculated using the volume which is common Metabolite Summary ClT = KV ClR = keV Clm1 = km1V Clm2 = km2V In this case Clm2 is the clearance of parent drug through the process of creating metabolite M2… not the clearance of metabolite M2!
1-C: Renal and Hepatic Elimination Since K = ke + km1 + km2 + kNR and ClT = ClR + Clm1 + Clm2 + ClNR when a metabolite is excreted completely into the urine… Metabolite Summary Ame0-∞ km Clm DoseIV K ClT ------------ = ----- = ----- * Amount of metabolite should be considered on a molar basis or be corrected for molecular weight.
1-C: Renal and Hepatic Elimination Metabolite Summary
1-C: Renal and Hepatic Elimination Consider Clopidogril Clopidogril has of an active metabolite with and known hlf-life of 8 hrs, that is shorter than the parent compound (24hr+), the elimination of the metabolite will be rate limited by the elimination of the parent compound (if you give the parent compound, metabolites will appear to have half-lives which are NEVER shorter than the parent compound ... but if you give the metabolite IV you see its actual half-life – 8 hr). This will explain the CPS's discussion of half-life vs. pharmacologic half-life ... and so steady state is determined by the slowest exponential in the mix ... the half life of clopidogrel.