Download
1 / 12
120 likes | 137 Views
This study examines the performance of Pharmacy and Therapeutics Committees (PTCs) in Thai hospitals during a period of healthcare reform, and explores ways to improve PTC performance through the development of practical performance indicators. The results highlight the need for a responsible organization to support and monitor PTCs, as well as the importance of effective PTC Chairpersons and collaboration among PTCs for decision-making. This research provides valuable insights for hospitals aiming to enhance rational drug use activities.

E N D
Background • In Thailand, hospitals under the Office of the Permanent Secretary were first required to establish Pharmacy and Therapeutics Committees (PTCs) in 1987. • A Manual of Drug Administration (1987) listed the expected structure, roles and responsibilities of PTCs. • Since 1997, Thai hospitals have faced economic crisis, quality improvement and accreditation, universal coverage health reform and structural change in the Ministry of Public Health (MoPH).
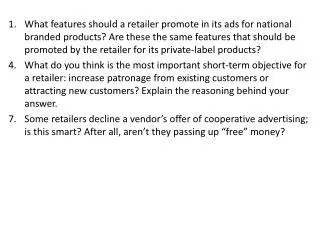
Objectives • To examine PTC performance during this period of change and reform. • To determine the opinion of the PTC Chairpersons and the PTC Secretaries about defining good PTC performance, ways to improving PTC performance, and possible PTC performance indicators. • To create a Manual that provides more practical help on rational drug use activities, including performance indicators.
Sample & methods • Seventeen hospitals (2 regional hospitals, 3 provincial hospitals, and 12 district hospitals) in 4 regions of Thailand. • Ten key informants who were the Chairperson, the Secretary or members of the PTC were interviewed. • Fifteen key informants who involved with PTC or who are responsible for drug information centers were interviewed. • Questionnaires were distributed to 452 PTC Chairpersons and Secretaries respectively in 25 regional hospitals, 67 provincial hospitals and 360 district hospitals. • Eight key participants who were PTC stakeholders participated in a focus group. • PTCs in 3 regional hospitals were observed.
Questionnaire results (1) • The questionnaire response rate was 36% from PTC Chairpersons and 66% from Secretaries. • Around 90% of PTC Chairpersons were Hospital Directors and 90% of Secretaries were Heads of Pharmacy Department. • The average of the number of PTC members in regional, provincial and district hospitals was 19, 20, and 10 members, respectively. • There were only 2-3 PTC meetings in regional or provincial hospitals and only 1-2 PTC meetings in district hospitals during each fiscal year (from 1996-2002).
Questionnaire results (2) • The most important PTC performance indicators suggested by all PTC Chairpersons: • Is PTC responsible for considering and approving allocation of drug budget proposed by the Pharmacy section? • Does PTC have a document providing criteria for addition and deletion of drug in the hospital drug list? • Does PTC have a policy to develop or implement Clinical Practice Guidelines for common problems such as acute respiratory infection, diarrheal diseases, hypertension, diabetes, epilepsy, and antibiotic prophylaxis, etc.? • Does the PTC monitor Pharmacy drug dispensing to ensure it followswritten standards of pharmacy professional practice? • Does PTC conduct satisfaction surveys on hospital staff to receive feedback on PTC performance?
Questionnaire results (3) • The most important PTC performance indicatorssuggested by PTC Secretaries: • Does a document identifying goal, committee, objectives, and functions of PTC exists? • Is PTC authorised to select drugs to be included and excluded in the hospital drug list? • Does PTC monitor the percentage of drugsused outside hospital drug list? • Does the PTC monitor Pharmacy drug dispensing to ensure it followswritten standards of pharmacy professional practice? • Does PTC have a policy to conduct satisfaction of patients/clients on the hospital treatment service?
Questionnaire results (4) • When asked about the most important factor needed for the development of an effective PTC: • the Chairpersons said it was an effective PTC Secretary; while • the Secretaries said it was an effective PTC Chairperson. • When asked about external factors that can contribute to improved performance of PTC both PTC Chairpersons and Secretaries in all hospitals agreed that the most important aspect was: • a national collaborative drug information center as a hub for information exchange between PTC for a decision making purpose. • In addition, PTC Chairpersons and PTC Secretaries in regional hospitals noted that: • defining the function of PTC in the hospital accreditation criteria would be helpful.
Results (5) • The retrospective document review, in-depth interviews, a focus group and participant observation noted that: • Under new structure of Ministry of Public Health, there was no distinctive responsible organization who support and monitor PTCs. • Some hospitals had not updatedinformation about new PTC members, functions or responsibilities. • Most PTC activities still focused on drug selection and controlling drug budget. Activities on rational drug use were few. • Many PTCs had not set their own specific goals, objectives, role and responsibilities. • Often PTCs had no working plan and there wasalso no orientation about goal, objectives, role and responsibilities for PTC members. • Many suggested the need for a responsible organization (perhaps under the Department of Health Service Support) that would assist PTCs by: • Updating Manual of PTC roles and responsibilities; • Providing opportunities for PTC networking e.g. by web site &/or E-mail discussion groups; • Providing information for PTC to make decisions; • Supporting the incorporation of PTC performance indicators in hospital accreditation (Bureau of Inspection & Evaluation &/or The Institute of Hospital Quality Improvement& Accreditation); • Encouraging Universities to provide educational programs.
Summary • PTCs at all levels of hospital focused their activities on drug selection and budget as this was the main focus of the 1987 “Manual”. • There were limited numbers of meetings of PTCs (1-2 in district hospitals; 2-3 in regional or provincial hospitals). • The recommended PTC performance indicators were the number of PTC meetings and the number of drug items in hospital drug lists. • Suggestions for improving PTC performance: • Setting a responsible organization; • Encouraging educational programs in universities; and • Providing national drug information center and PTC networking.
Conclusion & Policy Implications There is a need for a responsible organization (perhaps under the Department of Health Service Support) that would assist PTCs by: • Updating a Manual regarding PTC roles and responsibilities; • Providing opportunities for PTC networking e.g. by web site &/or E-mail discussion groups; • Providing information for PTC to make decisions; • Supporting the incorporation of PTC performance indicators in hospital accreditation monitored by: • Bureau of Inspection & Evaluation &/or • Institute of Hospital Quality Improvement; • Encouraging Universities to provide PTC educational programs.