Download
1 / 12
120 likes | 133 Views
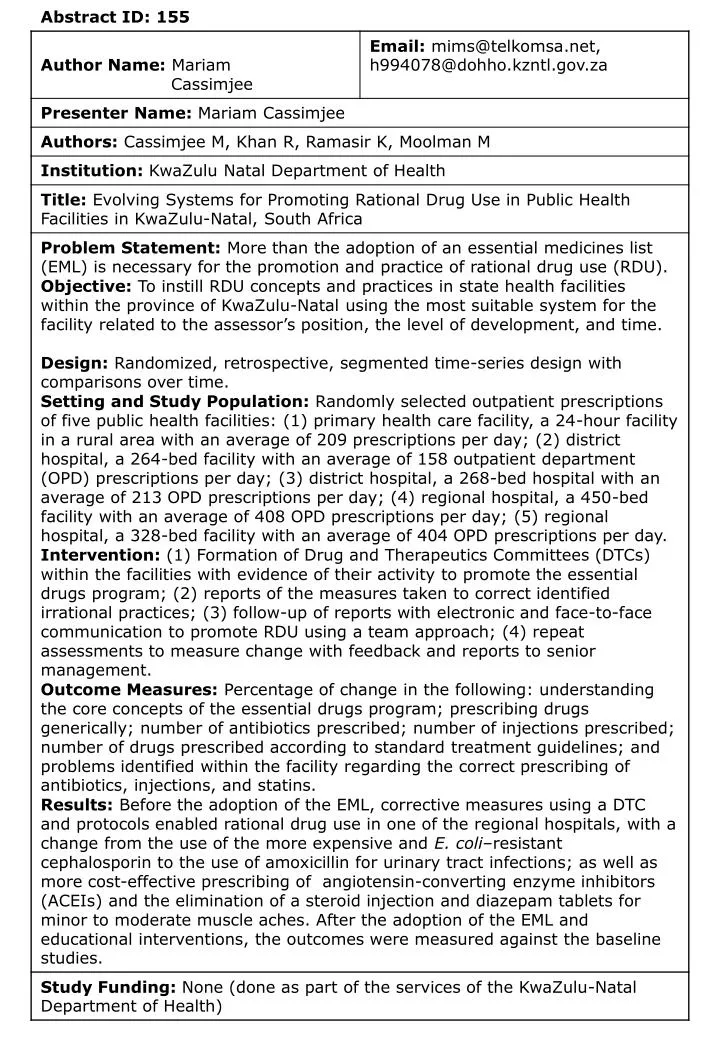
This study examines the evolution of drug use patterns from 1994 to 2004, focusing on the impact of interventions like drug utilization reviews, essential medicine lists, and adherence to standard treatment guidelines. Results from baseline assessments and post-intervention evaluations are analyzed to assess improvements in rational drug use practices.

E N D
Phases in Pursuing Rational Drug Use (RDU) The study spans over 1994 to 2004 of drug use patterns in pursuing. • Prior to 1996: Medicines were selected off the Provincial Medical Supplier’s catalogue. There existed an open and a restricted code with a number of choices for prescribing within a class of drugs. Marketing forces were strong and prevailed over the prescriber’s pen. • March 1996: A DTC was formed which initially served 3 hospitals and spread to the district. The purpose of the DTC: to advise on drug use, develop STGs and protocols for antimicrobials. • May 1996: The PHC Essential Medicine List (EML) arrived. Did it bring change for the better? Was there strong trends to adherence? • May 1999:The EMP with an EML and STGs for all levels of healthcare was launched. Study Question: Four years after the launch of the EMP, is there compliance or is more than an EML required for the promotion and practice of RDU?
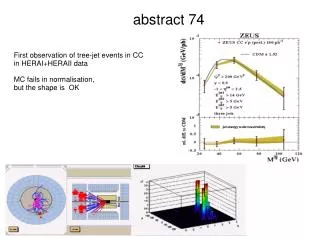
Av Monthly Usage Costs of Amoxycillin & Cephradine RE G I O N A L HO S P I T A L Regional Microbial Resistance Numbers E.Coli resistant to Cephalo-sporin amongst resistant orgs.
Pre-DTC or EML/STGs • Many drugs prescribed with not many questions asked! • DTC intervention: • Drew up a STG for the treatment of muscle aches effected changes with restriction on diazepam tablets, diclophenac and betamethasone injs.
Av Monthly Usage of Long Acting ACEIs (not standardisedfor equivalent doses) • The many long acting ACE-inhibitors afforded prescribers the use of many expensive choices! Both Perindopril and Ramipril were mostly used! • To curtail unwarranted expenditure and marketing influences, an EML with STGs introd-uced in May 1999 made a logical progression to RDU.
Baseline Indicator Study in OPDs: August 2003 Alarming baseline results of August 2003, using WHO indicators and a questionnaire to determine understanding the core concepts of the EMP programme, at a PHC clinic, a district hospital and at a regional hospital were noted.30 randomly sampled retrospective prescriptions for the sample size in each facility were used. The results were compared six months later to determine progress after interventions. Interventions After Baseline • Reports of the baseline evaluations, furnished to the facility clinical manager, included:- • Drug utilisation reviews (DURs) for problematic drugs to verify usage • Recommendations with respect to all aspects of the tests • Data on how to investigate drug use in health facilities • Strategies to monitor progress or regression
Strategies Used for Correction • Top management involvement for endorsement of process and for referee function. • Communications broadened: Email, telephonic & face-to-face support. • Audits: Inputs from manager to identify possible misuse/irrational prescribing • Measure or map the outcomes • Facility to determine the process to follow to correct problem from recommendations • Of paramount importance: the facility’s management is accountable for the quality of their service delivery and budgets. Their autonomy was therefore honoured by allowing them to decide on their interventions and processes to follow for addressing the identified problems. It also served as empowerment for the service and improved networking and communication.
Results of Pilot Sites: Baseline (8/2003) & Post (3/2004) Study KEY: Scores to be read with compliance to the STGs. Determines correct from incorrect usage. • =Area of Concern • = Marked Improvement after intervention • = Some Improvement after an intervention = Change in person answering questions. = to be read with compliance to STGs mostly correct usage for STIs
Discussion • The baseline results as depicted in red print were alarming. • First concern: Reasons for the gaps in know-ledge of the core concepts of the EMP & HPT STGs? Is there need to market the EMP more comprehensively in structured workshops? • RDU of antibiotics especially at PHC level: The Provincial Medical Suppliers were unable to keep up with the demand of Amoxycillin suspension in June 2003. This raises questions about the judicious use of antibiotics, more so by the fact that in the post baseline test sampling of 30 prescriptions in the district hospital, there were 10 prescriptions with antibiotics, of which one was resistant to amoxyciilin! • The need for research into amoxycillin resistance from PHC up the line seems warranted especially in view of the fact that the recently amended STGS for otitis media advocate the use of amoxyciilin. • +ve change: from 3.9% to 83.3% in the use of statins according to the STGs, training of medical officers to prescribe correctly with monitoring to ensure patient safety.
Distant Support - District Hospital • Baseline DUR for the statins (01 Jan 2003 to 01 July 2003) high usage • Problems identified: - • Prescribed outside the specialist prescriber level and outside STGs. • Non-drug measures & biochemical monitoring not followed. • Total cost over 7 months = R18,851 per month. Results - Statin Usage Support: young proactive Pharmacy Manager at a Distant District Hospital. Electronic communication: furnished strategies and DURs corrections achieved. Correct practices: moderate hypercholesterol- aemia treated with a generic simvastatin of more than 50% in expenditure with no compromise to the patient.
Conclusions • Almost 5 years after the launch of the EMP, non compliance was evident by the low scores. • An EMP with EML & STGs do not in themselves promote RDU • Appropriate interventions for the province & its health facilities, considering their level of development, physical accessibility, busy personnel schedules and demands are very necessary • More research into bridging gaps with respect to the implementation of the EMP is necessary • Therefore…........
Systems Needed to Promote RDU • An EMP with EML & one set of STGs • DTCs at all levels: National, provincial, districts and at health facilities. • Promoters, educators and marketers • Dedicated provincial person/s to promote, evaluate & assist district teams using an ambassadorial approach. • To facilitate educational workshops within establishments to bridge gaps and build in continuity for annual and other changes in staff • Finely tuned communication systems bulletins, minutes of meetings, network groups, electronic and face-to-face. • Human monitors based provincially, within the districts and health facilities. • Accountable management team within health facilities to perform audits and feedback. • Ongoing vigilance and research into antimicrobial resistance patterns at all levels of care.