Download
1 / 41
430 likes | 775 Views
Introduction to Survival Analysis. Utah State University January 28, 2008 Bill Welbourn. Objectives of this Talk. Clarify what survival data is. Explain what makes survival data special. Example 1 – Survival estimation for a single population.

E N D
Introduction to Survival Analysis Utah State University January 28, 2008 Bill Welbourn
Objectives of this Talk • Clarify what survival data is. • Explain what makes survival data special. • Example 1 – Survival estimation for a single population. • Example 2 – Survival comparison for two populations via infant ALL data. • Provide motivation for the need of “special” methods for analyzing survival data.
Objectives of this Talk (cont) • The notion of risk estimation for survival data, the Cox-Proportional Hazards Model. • Example 3 – Infant ALL data revisited, analyzed using Cox-Proportional Hazards Model.
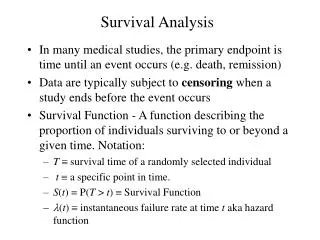
What is Survival Data? • Data that deal with the time until the occurrence of any well-defined event. • Binary response which does not have to be death/survival.
Examples of Events • Death • Response to a treatment • Development of a disease in someone at high risk • Resumption of smoking by someone who had quit • Cancellation of service by a credit card customer • Relapse of a patient in whom disease had been in remission
Complete Data • The value of each sample unit is observed or known. • Ex.) Compute the average test score for a sample of 5 students: 90, 80, 76, 85, 82.
Why is Survival Data Special? • Censored data: The event of interest may not be observed or the exact times-to-event of all the units are not known. Examples: • The event of interest is death, but at the time of analysis the patient is still alive. • A patient was lost to follow-up without having experienced the event of interest.
Examples (cont) • The event of interest is death caused by cancer. A patient may die of an unrelated cause, such as an automobile accident. • A patient is dropped from the study without having experienced the event of interest because of a major protocol violation.
Types of Censoring • Right censoring: a survival time is not known exactly but known to be greater than some value.
Types of Censoring (cont) • Left censoring: a failure time is only known to be before a certain time. Ex.) Event of interest: development of a disease. At the time of examination, a 50-year-old participant was found to have already developed the disease of interest, but no record of exact time.
Types of Censoring (cont) • Interval censoring: Objects of interest are not constantly monitored. Event of interest is known to have occurred between times a and b. Ex.) At age of 45, the patient did not have the disease. His age of diagnosis was between age 45 and 50.
Survival Estimation • Example 1 - A hypothetical clinical trial: Suppose that 10 patients enroll in a clinical trial at the beginning of 1988. During 1988, 6 patients die. At the beginning of 1989, 20 additional patients enroll in the trial. During 1989, 3 patients who enrolled in the trial at the beginning of 1988 die, and 15 patients who enrolled in the trial at the beginning of 1989 die. We are asked to estimate the one year and two year survival for these patients.
Survival Comparison • Example 2 - For acute lymphoblastic leukemia (ALL) in children, a small percentage of approximately 3% in this age range are diagnosed in the first year of life – referred to as infant ALL. • Generally the outcome for infant ALL is much poorer than that for other children, where about 75% go into a quick remission and never have their disease return (i.e., are cured).
Survival Comparison (Ex 2 cont) • For infant ALL probably 65% will die of their disease. While the outcome of ALL in these very small babies is not good, there is nevertheless substantial known heterogeneity in outcome based on patient characteristics – some subgroups doing much better and some much worse than the general outcome in infants. • In this exercise, we will examine if survival among ALL infants differs, depending on time of diagnosis (0-5 mo. vs. 6-11 mo.).
Survival Comparison (Ex 2 cont) • Hypothesis test setup: Null states that survival among ALL infants is the same, irrespective of the age of diagnosis. Alternative states that survival among infants diagnosed with ALL at 0-5 months is a constant scaled power (at any follow-up time) of the survival among infants diagnosed with ALL at 6-11 months. • More precisely, the alternative states that the hazard rates for the two infant ALL groups are proportional through time.
Structure of Survival Data • The following SAS output provides an overview of collected survival data.
Survival Comparison (Ex 2 cont) • To test these hypotheses, we use the Log-Rank Test.
Survival Comparison (Ex 2 cont) • The Log-Rank Test from SAS’ Proc Lifetest yields a p-value of 0.0057. There is evidence in this case to reject the null hypothesis. These data indicate that there is a statistically significantly difference in survival among children diagnosed with ALL at 0-5 months when compared to children diagnosed with ALL at 6-11 months (p<0.01). The data suggest that survival is better among children diagnosed with ALL later in infancy.
Survival Comparison (Ex 2 cont) • Assess Goodness-of-Fit (PH assumption).
Confounding Factors • Recall, a confounding factor for an association of interest – in this case, the age at diagnosis/survival relationship – must itself be associated to the outcome of interest (survival) and to the exposure of interest (age at diagnosis). • Let’s examine if abnormality for CHR11Q23 is a confounding factor for our example.
Confounding Factors (cont.) • To assess whether CHR11Q23 is associated with survival, we use the Log-Rank Test. SAS reports a p-value <0.01. These data indicate that there is a statistically significantly difference in survival among children with an abnormality at the CHR11Q23 loci compared to children without the abnormality (p<0.01). The data suggest that survival is better among children without the abnormality.
Confounding Factors (cont.) • To assess whether CHR11Q23 is associated with age at ALL disgnosis, we use Categorical Data Analysis. These data indicate the odds of CHR11Q23 abnormality among children diagnosed with ALL at 0-5 months is 2.78 times those among children diagnosed with ALL at 6-11 months (95% CI for OR, 1.19 – 6.48).
Confounding Factors (cont.) • Thus, the data suggest that CHR11Q23 is associated to both survival (outcome) and to age of ALL diagnosis… CHR11Q23 appears to be a confounder, and so we should control for the factor in the analysis. • After controlling for CHR11Q23, these data still suggest that survival is better among infants diagnosed with ALL later in infancy, but the evidence of the association has decreased (p=0.03).
Why the use of “Special” Statistical Methods forSurvival Data? • More precisely, since we have a binary response, why not use categorical data analysis methods (e.g., 2xC contingency tables, logistic regression) to analyze survival data?
“Special” Methods (cont) • Log-Rank Test and the Score Test from Logistic Regression essentially equivalent when all censored observations equal the maximum follow-up time. • Biased results could arise from the use of categorical data analysis methods, if uniform censoring through follow-up time in one group occurs and censoring at the maximum follow-up time for the second group occurs.
“Special” Methods (cont) • In utilizing categorical data analysis methods, uniform censoring through follow-up time in both groups could lead to bias toward the null hypothesis. • If censoring occurs at the beginning of the follow-up time for each group, utilizing categorical data analysis methods could lead to bias toward the alternative hypothesis.
“Special” Methods (cont) • If censoring does not occur, categorical data analysis methods cannot be applied. • In summary, survival analysis methods exist to handle the censoring of observations.
Risk Estimation for Survival Data • Log-Rank Test provides a means in testing for an association in survival. Cox-Proportional Hazards (CPH) Model provides a regression extension so that risk estimation in survival can be made. • Risk estimate for CPH Model is the hazard ratio.
GLM versus CPH Model • GLM – Parametric Models: • CPH – Semi-parametric Model:
Survival Comparison (CPH) • Example 3 – Let’s revisit the infant ALL data and analyze using the CPH Model. • Null hypothesis states that the hazard rate among ALL infants is the same, irrespective of the age at diagnosis. Alternative states that the hazard rate (at any follow-up time) among infants diagnosed with ALL at 6-11 months is a constant multiple of the hazard rate among infants diagnosed with ALL at 0-5 months.
Survival Comparison (Ex 3 cont) • To test these hypotheses, we use the Cox-Proportional Hazards Regression Model. • The CPH Model: • Model under the null:
Survival Comparison (Ex 3 cont) • Model under the alternative: • SAS’ Proc Phreg reports the p-value from the Likelihood Ratio Test to be 0.0057. Note that this result is essentially equivalent to the Log-Rank Test. This is expected as the hypotheses are the same for the CPH Test and the Log-Rank Test.
Survival Comparison (Ex 3 cont) • These data indicate the risk of death among infants diagnosed with ALL at 0-5 months is 2.10 times that of infants diagnosed with ALL at 6-11 months (95% CI for RR, 1.23 – 3.60).
Survival Comparison (Ex 3 cont) • Survival curves from SAS’ Proc Phreg:
Survival Comparison (Ex 3 cont) • Assess Goodness-of-Fit (PH assumption).
Confounding Factors Revisited • As with the Log-Rank procedure, we can control for confounding factors in the CPH Model. • The interpretation of the RR, models that of other regression techniques.
Adjusted RR Interpretation • After controlling for CHR11Q23 abnormality, these data indicate the risk of death among infants diagnosed with ALL at 0-5 months is 1.82 times that of infants diagnosed with ALL at 6-11 months (95% CI for RR, 1.05 – 3.15).