Download
1 / 16
160 likes | 183 Views
Best Practices in Healthcare Financing: Sri Lanka Case. Ravi P. Rannan-Eliya ECOSOC Annual Ministerial Review – Regional Ministerial Meeting on Financing Strategies for Health Care 16-18 March, 2009 Colombo, Sri Lanka. WB Good Practices in Health Financing. Low healthcare spender.

E N D
Best Practices in Healthcare Financing: Sri Lanka Case Ravi P. Rannan-Eliya ECOSOC Annual Ministerial Review – Regional Ministerial Meeting on Financing Strategies for Health Care 16-18 March, 2009 Colombo, Sri Lanka
Formative origins in 1930s • Democracy in 1931 • Made government accountable to people • Income tax introduced • Free education • Autonomy from foreign influence • Self-rule with freedom to find our own way • Adequate resources • Relatively good tax base • Economic crisis and epidemics • Impact of 1930s Global recession and 1934 Great Malaria Epidemic
Consequences • High priority given to risk protection • High allocation of budget to inpatient care and hospitals (>75%) • Emphasis on physical access over consumer quality • Extensive network of rural facilities • Pro-poor government spending • Removal of financial barriers • Abolition of user fees (1951)
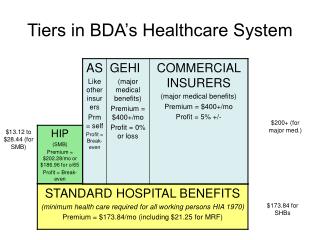
but a third model • Developing countries cannot afford UK NHS (“Beveridge”) model • Cost of government financing free care for all: 5-8% of GDP • Actual government budgets: 2-3% of GDP • So only able to pay for 40-60% of overall needs through public financing • Typical outcome is that limited public services are captured mostly by rich, leaving poor without services • Rationing through spatial barriers, or informal costs • Sri Lanka has solved this by successful mix of public and private financing and provision • Public services universal but used more by poor • With public spending focusing on insurance function
With self-selection of rich into private sector Use of public and private inpatient services by income quintiles
Key Messages • Accountability to people is critical • Government must provide insurance through hospital care • Improving efficiency is critical for expanding coverage • Never give up on public sector • Manage the financing gap by prudent use of voluntary private care