Download
1 / 60
680 likes | 982 Views
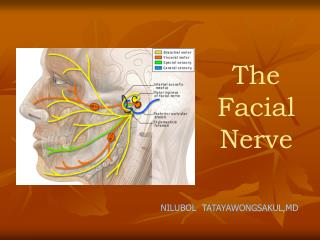
Facial Nerve Paralysis. Melanie Giesler, DO. Anatomy. Anatomy. The motor nucleus of the facial nerve lies deep within the reticular formation of the pons where it receives input from the precentral gyrus of the motor cortex, which innervates the ipsilateral and contralateral forehead.

E N D
Facial Nerve Paralysis Melanie Giesler, DO
Anatomy • The motor nucleus of the facial nerve lies deep within the reticular formation of the pons where it receives input from the precentral gyrus of the motor cortex, which innervates the ipsilateral and contralateral forehead. • Cerebral cortical tracts also innervate the contralateral portion of the remaining face. • Accounts for the sparing of the forehead motion in supranuclear lesions of the facial nerve
Differential DiagnosisAcute facial palsy • Infection • Herpes Zoster Oticus (Ramsey Hunt Syndrome) • Lyme disease • Acute Otitis media +/- mastoiditis • Congenital • Treacher Collins syndrome • Mobius syndrome • Trauma • Temporal Bone fracture • Barotrauma • Metabolic • Diabetes • Hypothyroidism • Vascular • Benign intracranial hypertension • Neoplasm • Facial neuroma • Acoustic neuroma • Toxic • Thalidoide • Iatrogenic
Physiology of Nerve Injury • When an axon is injured, biochemical and histological changes occur in the cell body proximal and distal to the site of the injury. • Severity of the changes depend upon: • distance from the injury to the cell body (proximal injuries usually more severe than distal injuries), • type of injury (crush injuries more severe than clean transections) • age of the patient (older individuals sustain more severe injury than younger patients) • nutritional and metabolic status of the patient.
Sunderland classification of peripheral nerve injury Neurapraxia Axonotmesis Neurotmesis
First Degree • Neuropraxia • localized conduction block in the nerve with the nerve fibers responding to electrical stimuli proximal and distal to the lesion, but not across the injured segment. • Axonal continuity is preserved, wallerian degeneration does not occur, and recovery is usually complete. • Arm “falling asleep”
Second Degree • Axonotmesis • Disruption of the axon into proximal and distal portions with interrupted axoplasmic flow. • Wallerian degeneration occurs within 24 hours in the distal portion of the axon and to a slight degree in the proximal portion. • The connective tissue elements remain intact, however, and the axon may regenerate at a rate of 1 mm/day to the original end organ with the potential for complete recovery.
Third Degree • Endoneurotmesis • Endoneurium and axon are destroyed, but the perineurium remains intact. • Wallerian degeneration occurs. • Axons may regenerate, but can be blocked by scar tissue. • This will result in partial reinnervation. In addition, misdirection of fibers can occur with resultant synkinesis (abnormal mass movement of muscles which do not normally contract together) and incomplete recovery.
Fourth Degree • Perineurotmesis • Only the epineurium remains intact, while the axon, endoneurium, and perineurium are disrupted. • Wallerian degeneration occurs, and there is much greater chance for aberrant regeneration, synkinesis, and incomplete recovery. • Analogy of cord with fibers inside broken but insulation portion remains intact
Fifth Degree • Neurotmesis • Complete disruption of neural continuity. • Without careful repair, there is little to no chance of regeneration and recovery • Axonal sprouts may escape the confines of the nerve sheath and produce painful neuromas adjacent to the injured nerve. • Except in cases of complete transection, nerve injury is usually a combination of degrees of injury.
Clinical Evaluation • History • Onset of the paralysis (sudden vs delayed) • Duration, and the rate of progression. • It is especially important to determine whether the paralysis is complete verses incomplete. • Patients should be questioned regarding previous episodes, family history, associated symptoms (hearing loss, otorrhea, otalgia, vertigo, headaches, blurred vision, parasthesias), associated medical illnesses (diabetes, pregnancy, autoimmune disorders, cancer), history of trauma (recent or remote), and previous surgery (otologic, rhytidectomy, parotidectomy).
Physical Examination • Complete head and neck examination must be performed, including microscopic examination of the ears, careful palpation of the parotid glands and neck, ophthalmologic examination (r/o papilledema), auscultation of the neck ( r/o carotid bruits), and a thorough neurological examination. • It is important to assess the degree of voluntary movement present in order to document the grade of facial paralysis as described in the House classification system
Central vs Peripheral • Supranuclear (central) lesions produce contralateral voluntary lower facial paralysis. The frontalis muscle is spared because of the bilateral innervation as described previously. • Emotional response (facial motion on laughing or crying) may also be preserved with central lesions. • Presence of Bell's phenomenon (upward outward turning of the eyeball as the patient attempts to close the eyelids) indicates a peripheral lesion.
Work Up • Any patient presenting with facial paralysis should undergo formal audiological testing, including pure tone, air and bone conduction, speech discrimination, reflexes, and tympanometry. • If asymmetry is found on the audiogram, an ABR and/or MRI should be obtained. Electronystagmography (ENG) is usually not indicated unless vertigo or other balance disturbance is part of the clinical picture.
Radiologic Evaluation • May be undertaken in patients with a history of recurrent paralysis, associated neurological symptoms, suspected CPA lesions, concurrent otologic findings (AOM, COM, suspected cholesteatoma), history of trauma, gradually developing facial nerve paralysis, atypical presentation, or if patients show no evidence of recovery after one month from onset.
Radiologic Evaluation • Gadolinium enhanced MRI is superior for soft tissue evaluation and will usually reveal the inflammation and edema associated with Bell's palsy and with Herpes Zoster oticus. It is also considered to be the procedure of choice to rule out a cerebellopontine angle tumor or other brain tumors. • High- resolution computed tomography provides excellent bony assessment and is the study of choice to rule out a temporal bone fracture, or to evaluate the middle ear and mastoid.
Electrophysiologic Testing • These tests are useful for patients with complete paralysis for determining prognosis for return of facial function and the endpoint of degeneration by serial testing. • They are most useful when considering decompression surgery and are of no value in patients with incomplete paralysis.
Electrophysiologic Testing • Nerve excitability test (NET), maximal stimulation test (MST), and electroneuronography (ENoG) are most useful in the degenerative phase. • These tests will give normal results during the first 72 hours after injury due to the stimulating and recording electrodes both being distal to the site of the injury. • After 3 - 4 days, the nerve degeneration reaches the site of stimulation and useful results will be obtained. • These tests can only be used for unilateral paralysis because all three involve comparison to the contralateral side which must be normal for valid results.
Nerve Excitability Test • Nerve excitability test (NET) is the most commonly used secondary to the low cost, readily available equipment, and ease of performance. • This test involves placement of a stimulating electrode over the stylomastoid foramen. The lowest current necessary to produce a twitch on the paralyzed side of the face (threshold) is compared with the contralateral side. A difference of greater than 3.5 milliamps indicates a poor prognosis for return of facial function. • The major draw back to the use of this test is its subjectivity, with reliance entirely on a visual end point. In addition, since such a small amount of current is used with this test, a few intact axons may give a visible response leading the clinician to predict a good prognosis, when in reality most of the fibers are degenerating
Maximum Stimulation Test • Maximum stimulation test (MST) is a modified version of the NET. A maximal stimulus is used to depolarize all facial nerve branches. • The paralyzed side is then compared to the contralateral side and the difference is graded as equal, slightly decreased, markedly decreased, or absent. • Testing begins on the third day post onset and is repeated periodically until return of facial function or absent response. An equal or slightly decreased response on the involved side is considered favorable for complete recovery. • An absent or markedly decreased response denotes advanced degeneration with a poor prognosis. The response to this test becomes abnormal sooner than the response to the NET and is therefore considered superior. However, like the NET, this test is also subjective.
Electroneurography (ENoG) • Considered to be the most accurate prognostic test because it provides an objective, qualitative measurement of neural degeneration. • The facial nerve is stimulated with an impulse transcutaneously at the stylomastoid foramen using bipolar electrodes. The muscular response is then recorded using bipolar electrodes placed near the nasolabial groove. The peak to peak amplitude of the evoked compound action potential is considered proportional to the number of intact axons. • The two sides are then compared with the response on the paralyzed side of the face expressed as a percentage of the response on the normal side of the face. A reduction in amplitude on the involved side to 10% or less of the normal side indicates a poor prognosis for spontaneous recovery. A maximal reduction of less than 90% within 3 weeks of onset gives an expected spontaneous rate of recovery of 80 - 100%.
Electromyography (EMG) • Is of limited value early in the evaluation of facial paralysis because fibrillation potentials indicating axonal degeneration do not appear until 10 to 14 days post onset • EMG becomes important for assessing reinnervation potential of the muscle two weeks after onset. By using needle electrodes placed transcutaneously into the muscles of facial expression, muscle action potentials generated by voluntary activity can be recorded. • Electrical silence can indicate normal muscle in a resting state, severe muscle wasting and fibrosis or acute facial paralysis in the early stages. During normal voluntary contraction organized diphasic or triphasic potentials are seen. • Fibrillation potentials indicate degeneration of the neural supply to the muscle in question. Polyphasic potentials indicate reinnervation. These are important because they usually appear 6 - 12 weeks before clinical return of function.
Bell’s Palsy • Bell's palsy is the most common cause of facial paralysis and accounts for more than half of all cases. Traditionally, this was considered to be a diagnosis of exclusion after ruling out all other possible causes. • However, it has recently been considered a positive diagnosis if the following are present: unilateral weakness of all facial muscles of sudden onset, possibly associated with a viral prodrome, no evidence of central nervous system pathology, no evidence of a CPA lesion, no history of otologic disease.
Bell’s Palsy • Estimated to be 20 to 30 per 100,000, but appears to increase with age. • There is an equal male to female ration and a 3.3 times greater incidence in pregnant females. • The left and right sides of the face are equally involved, and less than 1% of cases are bilateral. • The recurrence rate is about 10% and can be ipsilateral or bilateral. Patients with diabetes have 4 - 5 times more risk of developing the disease. A family history is positive in about 10% of patients with Bell's palsy.
Bell’s Palsy • The most likely site of lesion in Bell's palsy is the meatal foramen (junction of the internal auditory canal portion of the nerve and the labyrinthine segment of the nerve), which is considered to be the narrowest portion of the fallopian canal. • MRI with gadolinium will usually show enhancement of the labyrinthine portion of the nerve. As the edema within the nerve increases, axonal flow and circulation are inhibited resulting in varying degrees of nerve injury (first, second, and third degree). • Patients who are most severely affected develop a high level of third degree injury which can result in the loss of endoneural tubules and misdirected axonal regeneration. Histological studies from patients with Bell's palsy who died of nonrelated causes reveal diffuse demyelination of the facial nerve with lymphocytic infiltrates
Bell’s Palsy • The prognosis for Bell's palsy is generally good with 85 to 90% of patients recovering completely within one month. • The remaining 15% progress to complete degeneration and will not usually show signs of recovery for three to six months. • The longer the time needed for recovery, the greater the probability of sequelae. • The single most important prognostic factor is the degree of paralysis. Patients with incomplete paralysis will recover with no sequelae 95% of the time
Bell’s Palsy • Patients may exhibit evidence of concomitant sensory cranial polyneuritis with otalgia or postauricular pain, dysacousis or hyperacusis, dysgeusia, decreased tearing or epiphora, and facial hypesthesias/dysesthesias of V or IX . • Although the exact etiology of Bell's palsy is still unclear, most clinicians believe that herpes simplex infection is the most likely agent. This belief is supported by an increased incidence of HSV antibodies in patients with Bell's palsy when compared to age-matched controls
Bell’s Palsy • The treatment of Bell's palsy is variable, ranging from observation to surgical decompression. Regardless of treatment given, all patients must be counselled regarding proper eye care to prevent exposure keratitis. • Patients should use natural tears liberally during the day and should place lacrilube ointment in the eye at night. • Taping of the eye lids during sleep may be helpful as well as the use of a moisture chamber. • Patients should avoid fans and dust, and should consider wearing eye protection when outside in the wind.
Management of Bell’s Palsy • Observation • Medical Treatment • Steroid • Anti-viral agents • Surgery • Decompression • Dynamic vs. static reanimation • Facial Rehabilitation
Trauma • Trauma is the second most common cause of facial nerve paralysis. Longitudinal fractures of the temporal bone make up 80% of all temporal bone fractures. • In this type, the fracture line extends along the longitudinal axis of the temporal bone resulting in an external auditory canal laceration, TM perforation, and possible ossicular disruption or hemotympanum. Facial nerve injury occurs in 10 to 20% of these fractures with the injury most common in the perigeniculate region. • Transverse fractures are much less common (20% of all temporal bone fractures). These fractures extend along the transverse axis of the temporal bone across the vestibule, resulting in sensorineural hearing loss, possible loss of vestibular function, and a 50% chance of facial nerve injury which is also usually in the perigeniculate region.
T-bone Fracture • For complete facial nerve paralysis with clinical evidence of a temporal bone fracture, obtain a high resolution CT scan/temporal bone protocol. • If an obvious fracture is present, surgical exploration of the facial nerve should be undertaken as soon as possible via either a transmastoid/translabyrinthine (+ SNHL) or transmastoid/middle fossa approach (- SNHL). • During exploration the nerve must be fully exposed in order to identify all injured segments, and remove any compression from fracture fragments. • The nerve sheath should be incised and any hematomas within the sheath must be carefully evacuated. • If complete transection of the nerve is found during exploration, a direct end-to-end anastomosis should be performed if possible.
T-Bone Fracture • For incomplete facial nerve paralysis or for delayed onset paralysis associated with a temporal bone fracture, facial nerve testing should be obtained on day 4 after onset. • If advanced degeneration has occurred, the nerve should be surgically explored and decompressed.
Herpes Zoster Oticus • Third most common cause of facial nerve paralysis. • This is a manifestation of a dormant varicella zoster virus reactivating in extramedullary cranial nerve ganglia during a period of decreased cell mediated immunity. • The prodromal symptoms are very similar to those seen in Bell's palsy, but are usually more severe. Symptoms include severe otalgia, facial paralysis, facial numbness, and a vesicular eruption on the concha, external auditory canal, and palate. • Patients may also have varying degrees of SNHL, vestibular symptoms, and associated cranial nerve symptoms.
Herpes Zoster Oticus • Laboratory evaluation will often show the rise and fall of antibody titers specific for the virus. The palsy is usually more severe and the prognosis much poorer compared to Bell's palsy. • Only about 50% of these patients regain normal facial function as opposed to 90% with Bell's palsy. The degeneration occurs more slowly, usually over three weeks instead of two. • Treatment includes steroids, valacyclovir 1 gm po tid, and proper eye care. Surgical decompression has not been proven beneficial but may be considered for ENoG showing greater than 90% degeneration.
Otitis Media • In patients with evidence of acute otitis media, dehiscences in the fallopian canal may serve as portals for direct bacterial invasion and inflammation along the nerve. • Facial paralysis may begin within a few days of onset of an acute otitis media and is usually incomplete. Treatment includes a wide myringotomy, drainage, and culture with antibiotic coverage for gram positive cocci and H. flu. • The facial palsy associated with acute otitis media generally resolves with aggressive management of the infection. • However, if a total paralysis is present, serial ENoG should be obtained. If axonal degeneration reaches > 90%, surgical exploration and decompression should be performed.
Chronic Otitis Media • Develop facial paralysis which is usually secondary to cholesteatoma or from inflammation/osteitis compressing the facial nerve. • In these cases a high resolution CT should be obtained, and surgery should be performed as soon as possible (tympanomastoidectomy, facial nerve exploration and decompression).
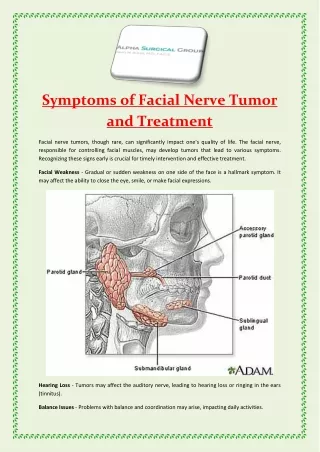
Tumors • About 5% of cases of facial nerve paralysis are caused by tumors. • Factors which should increase the clinicians suspicion of a possible tumor include: a slowly developing paresis over more than three weeks, facial twitching, additional cranial nerve deficits, recurrent ipsilateral involvement, associated adenopathy, or a palpable neck or parotid mass. • In these cases, MRI and CT should be obtained.
Tumors • The most common benign tumor causing facial nerve paralysis is a facial nerve schwanomma. • The most common malignant tumors causing facial paralysis are mucoepidermoid carcinoma and adenoid cystic carcinoma of the parotid gland. • The management of facial nerve paralysis caused by tumors depends upon the lesions location, size, and malignant potential and may include transposition of the nerve, division and reanastomosis, interposition grafting, and cranial nerve crossover. • After nerve grafts, the best possible result that can be expected is a House grade III paresis.
Melkerson-Rosenthal Syndrome • Rare disease that consists of a triad of symptoms: recurrent orofacial edema, recurrent facial palsy, and lingua plicata (fissured tongue). • The defining feature of this disease is the persistent or recurrent nonpitting facial edema that cannot be explained by infection, malignancy, or connective tissue disorder. • It usually involves the lips and buccal area and may involve the gingiva, palate, and tongue. • The lips become chapped, fissured, and red-brown in appearance and may develop permanent deformity after numerous recurrences. • Facial paralysis and lingua plicata occur in half of the patients. The complete triad is only present in 25% of these patients
Melkerson-Rosenthal Syndrome • The complete triad is only present in 25% of these patients. This condition usually starts in the second decade of life, and the manifestations usually occur sequentially (rarely simultaneously). • The etiology of this syndrome is unknown. Some consider it a variant of sarcoidosis secondary to biopsies of the lips which may reveal noncaseating granulomas. • Facial paralysis occurs in 50 to 90% of these patients and tends to be abrupt. A history of bilateral sequential paralysis and relapse after initial recovery is common. • The site of the paralysis usually corresponds to the facial swelling. Facial nerve decompression may be indicated if episodes of facial paralysis are frequent and progressive.