Download

1 / 39
400 likes | 689 Views
Depression. Depression. Known as a Mood/Affective Disorder Affect = emotions Major Types Bipolar Unipolar Seasonal Affective Disorder. Depression. Unipolar (major depression) Most common affective disorder 19 million Americans/year (17%)

E N D
Depression • Known as a Mood/Affective Disorder • Affect = emotions • Major Types • Bipolar • Unipolar • Seasonal Affective Disorder
Depression • Unipolar (major depression) • Most common affective disorder • 19 million Americans/year (17%) • 11 million clinical & major depression • 15% parasuicide • Good news…Most effectively treated
Depression Unipolar (major depression) Problems with diagnosis? Both a mental disorder & normal mood state
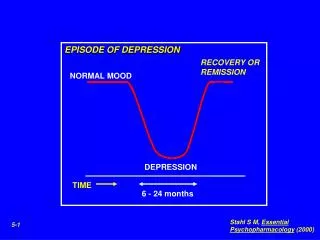
Depression Problems with diagnosis Reactive-Exogenous triggered by an obvious event Endogenous No trigger No obvious event Duration & Intensity
Anhedonia (experience pleasure) • Weight gain or loss • Hypersomnia, insomnia • Fatigue, loss of energy • feelings of worthlessness guilty • difficulty concentrating
Clinical Depression (5 symptoms) (2 symptoms)
Genetic Risk Concordance rate of 68% (monozygotic) Concordance rate of 15% (dizygotic) Family member = 10 tx more likely
Theories of Depression (Biological)
Most Dominant Theory of Depression Monoamine Hypothesis of Depression Depression is associated with an under activity at serotonergic and noradrenergic synapses (Indolamines & catecholamines)
Evidence in Support • CSF of depressed pt suicidal • low levels of 5HIAA • Post Mortem • brains from depressed pt (prefontal) • above avg # of 5HT & Norepi receptors • upregulation • Post Mortem Suicide • low 5HT • low Norepi
Evidence in Support • Tryptophan depletion in depressed • pt (Delgado, 1990) • Put on Low Trypto. Diet (salad, corn, gelatin) • Then, amino acid cocktail (no trypto.)…so hi • other amino acids • Trypto. Dropped! = relapse • -Healthy…no effect of diet or cocktail • …PET shows prefrontal cortex trypto less
Evidence in Support • Antidepressants Work!..so, monoamine • agonists • Monoamine Antagonist = depression • ex: Reserpine (Rauwolfia serpentina) • 100’s years ago used to • calm insanity • treat hi BP = 15% got depressed
Evidence Refuting the Monoamine Hypothesis • Antidepressants Work…in 80% of the • clinical population • …what’s up with the other 20%??? • -“Lag Time” • time it takes a drug to work in the • brain vs the time we see a behavioral • effect 3 to 4 weeks to see behave • effect…although in the brain
Evidence Refuting the Monoamine Hypothesis Neurogenesis Theory of Depression Dentate Gyrus: Hippocampus
Antidepressant increase neurogenesis in hippocampus Section of the dentate gyrus of the hippocampus, showing newly formed cells. These are the darker cells in the subgranular zone (SGZ), and they have been labelled with 5-bromo-2-deoxyuridine (BrdU), an analogue of thymidine. The histogram shows that various antidepressant treatments increase the number of new labelled cells. The treatments tested include electroconvulsive shock (ECS), the MAOI tranylcypromine (TCP), the SSRI fluoxetine (FLU), and the selective norepinephrine reuptake inhibitor reboxetine (REB). Santerelli et al, 2003, Science
Evidence Refuting the Monoamine Hypothesis Neurogenesis Theory of Depression
proliferation survival Exercise….
Treatment – Biochemical Therapies
Antidepressants • Monoamine Oxidase Inhibitors (MAOIs) • Tricyclics • Selective Monoamine Reuptake • Inhibitors (SSRIs)
Monoamines • Catecholamines: Norepinephrine • Indolamines: Serotonin
Monoamine Oxidase Inhibitors (MAOIs) - MAOIs block the enzyme monoamine oxidase… - MAO breaks down monoamines into inactive metabolites
MAOIs: • Iproniazid (eye-pron-eye-a-zid) • First antidepressant (1957) • - originally marketed as rocket fuel • - TX for TB • A flop!…serendipity intervened
MAOIs: • Isocarboxazid • Phenelzine • Tranylcypromine • Side effects: • hypertension (BP): headaches, sweating, • nausea, vomiting • Side effects represent drug interaction • drug X food • Tyramine – cheese, wine, licorice, raisins • MAO breaks down tyramine= too much • intracranial hemorrage (stroke)
MAOIs: • “Cheese Effect” • Pharmacist G.E.F. Rowe • wife was being treated with MAOI • headaches after eating cheese • Blackwell et al • found that cheese causes a large • increase in BP without MAO • increase in tyramine indirectly acts on sympathetic release of Norepi
Tricyclics Called tricyclics because chemical structure Includes 3-ring structure – 2 benzene rings & 1 central seven membered ring
Tricyclics works by preventing presynaptic reuptake
Tricyclics 1st tricyclic: Imipramine (Tofranil) serendipity! - Synthesized in 1948 as an antihistamine - Used in Schizophrenia – no help with psychosis but less depressed Side effects: (safer than MAOI) - block histamine receptors: produces drowsiness - block acetylcholine receptors: dry mouth, difficulty urinating - Na+ Channels: heart irregularities
Tricyclics • Appear to work better with: • - Early morning awakenings • - Loss of appetite • - Weight loss • Morning depression heightened • Contraindicated for Bipolar depression can trigger the mania
Second Generation: Selective Serotonin Reuptake Inhibitors (SSRIs) “Atypical” Antidepressants
SSRIs • Just Like the tricyclics but selective to • block serotonin uptake • Fluoxetine (Prozac) • -first on the market in 1980s • -most prescribed • -not more effective in tx depression • * fewer dangerous side effects • * effective in a wide range of • affective problems lack of self-esteem, fear of failure, OCD, Binge eating & purging (Bulimia)
SSRIs (Sertraline:Zoloft, Paroxetine:Paxil • (Fluvoxamine: Luvox, Citalopram:Celexa) • Side Effects: • SSRIs do not effect: • MAO – little risk of hypertension • Do not worry about food interaction However side effect: nervousness 25% nausea-10% nausea (Prozac & Zoloft) Priapism (trazadone) - protracted & painful penile erection Social anxiety disorder, PTSD, Panic disorder, OCD) ALSO: Selective Norepi Reuptake Inhibitors (Reboxetine)