Download
1 / 11
110 likes | 258 Views
Chronic diseases as tracer conditions in international benchmarking of health systems: the example of diabetes. Ellen Nolte 1 , Chris Bain 2 , Martin McKee 1. 1 European Centre on Health of Societies in Transition London School of Hygiene and Tropical Medicine, UK

E N D
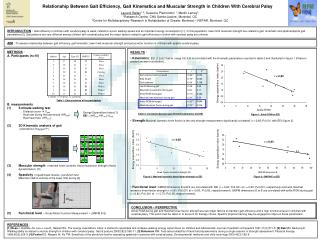
Chronic diseases as tracer conditions in international benchmarking of health systems: the example of diabetes Ellen Nolte1, Chris Bain2, Martin McKee1 1 European Centre on Health of Societies in Transition London School of Hygiene and Tropical Medicine, UK 2 School of Population Health, University of Queensland, Australia
Assessing health system performance • Health systems are complex with multiple functions • They must respond to varied health needs of the population with limited resources • They involve trade-offs, e.g. between prevention & treatment or primary & specialised care • It is unlikely that any system will perform well on all possible measures
How do countries compare? • Different models of health care provision • Differences at different levels • Approach: ‘probe disorders’ or ‘tracer conditions’ that capture certain elements of the health care system • Discrete and identifiable health problem • Evidence of effective, well-defined health care intervention • Natural history of condition varies with utilisation and effectiveness of health care • Sufficiently common
Diabetes as tracer condition • Optimal management requires • co-ordinated inputs from range of health professionals incl. primary care & specialists • access to essential medicines & monitoring equipment • active participation of informed patients • Can provide important insights into primary and specialist care, and into systems for communicating among them • Deaths (<45) considered ‘avoidable’ by timely and effective health care
SDR0-39 SIR0-14 Diabetes mortality (SDR0-39) and incidence (SIR0-14) SDR 0-39 SIR 0-14
Study design • Outcome measure: Mortality-to-incidence ratio • commonly used in cancer epidemiology as a crude indicator of cancer survival or “case fatality” • may be interpreted as an indicator of the overall quality of health care • Age-standardized incidence rates for ages 0-14 years (WHO DiaMond study, 1990-1994) • Age-standardised death rates from diabetes for ages 0-39 (WHO mortality database, 1994-1998) • Study population: 29 industrialised countries
Next steps • M/I ratio only an indicator of potential differences in health system performance & should stimulate detailed assessments to confirm whether the apparent variations are real and identify the reasons • Scrutinise data • Understand immediate causes of death • e.g. ~50% of deaths in Estonia & Latvia due to acute complications of diabetes compared to only 22% in Finland (Podar et al. 2000) • Understand processes of care
Conclusions (1) • M/I ratio for diabetes provides means of differentiating countries that appear to provide differing quality of care to people with diabetes and by extension to other chronic diseases • Further work is required to develop • a battery of performance indicators that capture other aspects of health system performance • instruments that can be used for detailed health system diagnosis once indicators suggest the presence of a problem
Conclusions (2) • International comparisons of health (care) systems have focused on what can most readily be measured, not what is necessarily important • While indicating the existence of a possible problem they provide few insights in how to respond • Tracer conditions offer approach to overcome some of these limitations • This study is an attempt to show how to shift the agenda on performance assessment to disorders such as chronic disease that are critically important