Download
1 / 16
160 likes | 250 Views
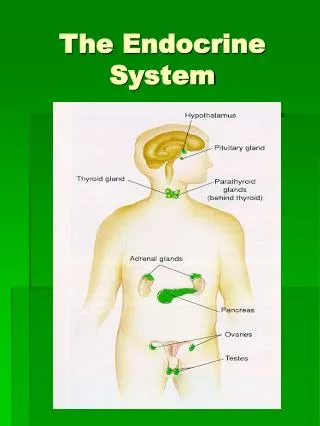
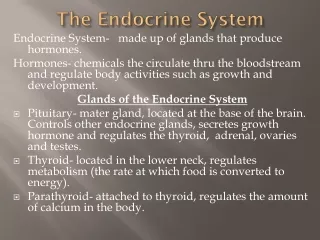
The Endocrine System. Pituitary Gland. Anterior pituitary Somatotrophs – GH Lactotrophs – prolactin Corticotrophs – ACTH, POMC, MSH Thryotrophs – TSH Gonadotrophs – FSH, LH Posterior pituitary – axonal processes from hypothalamus: Oxytocin ADH

E N D
Pituitary Gland Anterior pituitary Somatotrophs – GH Lactotrophs – prolactin Corticotrophs – ACTH, POMC, MSH Thryotrophs – TSH Gonadotrophs – FSH, LH Posterior pituitary – axonal processes from hypothalamus: Oxytocin ADH Clinical – Hyperpituitarism, Hypopituitarism, local mass effects – radiographic abnormalities of the sellaturcica, visual field abnormalities, elevated intracranial pressure, pituitary apoplexy
Pituitary Gland Hyperpituitarism – pituitary adenoma Most common cause is adenoma arising in the anterior pituitary Classified based on the hormone produced Functional or nonfunctional Microadenoma < 1 cm Macroadenoma > 1 cm Usually soft, well-circumscribed 30% invasive adenomas – no capsule Cellular monomorphism and the absence of a significant reticulin network distinguish pituitary adenomas from non-neoplastic anterior pituitary parenchyma Atypical adenomas – p53 mutations, aggressive
Pituitary Gland Prolactinomas Most frequent hyperfunctioning adenoma Amenorrhea, galactorrhea, loss of libido, infertility Tend to undergo dystrophic calcification Any mass in the suprasellar department may disturb the normal inhibitory influence of the hypothalamus (via dopamine secretion) on prolactin secretion resulting in hyperprolactinemia
Pituitary Gland Somatothroph adenoma Second most common GH stimulates the hepatic secretion of IGF-1 ( somatomedin C) Gigantism or acromegaly Failure to suppress GH production in response to a glucose challenge is one of the most sensitive tests for acromegaly
Pituitary Gland Corticotroph adenoma Cushing disease Nelson syndrome Gonotroph adenoma Thyrotroph adenoma Nonfunctioning pituitary adenoma Pituitary carcinoma ( <1% of all pituitary tumors)
Pituitary Gland Hypopituitarism Decreased secretion of pituitary hormones Hypofunction when > 75% of pituitary is lost or absent Causes – Tumors and other mass lesions, traumatic brain injury, subarachnoid hemorrhage, pituitary surgery or irradiation, pituitary apoplexy, ischemic necrosis and Sheehan syndrome, Rathke cleft cyst, empty sella syndrome, genetic defects, hypothalamic lesions, inflammatory or infections
Pituitary Gland Posterior pituitary syndromes DI SIADH Hypothalamic suprasellar tumors Gliomas Craniopharygiomas
Thyroid Gland Hyperthyroidism Hypermetabolic state caused by elevated circulating levels of free T3 and T4 Thyrotoxicosis Most common forms: Diffuse hyperplasia associated with Graves disease ( 85%) Hyperfunctionalmultinodular goiter Hyperfunctional adenoma of the thyroid
Thyroid GLand Clinical manifestations of hyperthyroidism Hypermetabolic state Overactivity of the sympathetic nervous system Warm, flushed skin heat intolerance Sweating Weight loss despite increased appetite Cardiac- tachycardia, palpitations, cardiomegaly, arrhythmias,CHF,cardiomyopathy Neuromuscular – tremor, hyperactivity, emotional lability, anxiety, inability to concentrate, insomnia, myopathy Ocular – wide staring gaze, lid lag Osteoporosis Thyroid storm Apathetic hyperthyroidism
Thyroid Gland Hypothyroidism Causes- Primary – Thyroid dysgenesis, Thyroid hormone resistance syndrome, postablative, Hashomoto’s thyroiditis, Iodine deficiency, drugs, dyshormonogenetic goiter Penred syndrome (+hearing loss) Secondary – Pituitary failure, Hypothalamic failure
Thyroid Gland Clinical manifestations: Cretinism – infancy or childhood, impaired development of the skeletal system and CNS, short stature and mental retardation Myxedema- older child or adult, slowing of physical and mental activity, fatigue, apathy, mental sluggishness, decreased sympathetic activity, non-pitting edema due to accumulation of matrix substances, decreased cardiac output
Thyroid gland Thyroiditis Infectious- acute or chronic Hashimoto – autoimmune; anti- thyroglobulin, anti-thyroid peroxidase antibodies, Painless enlargement with hypothyroidism in a middle- aged woman, inflammatory infiltrate, germinal centers, Hurthle cells Subacute (granulomatous or DeQuervain) - triggered by a viral infection, painful enlargement, transient Subacute lymphocytic (painless) – also post- partum, variant of Hashimoto Riedel – extensive fibrosis of thyroid and contiguous structures
Thyroid Gland Graves disease Hyperthyroidism Infiltrative ophthalmopathy exothalmos Localized, infiltrative dermopathy pretibial myxedema Antibodies: Thyroid-stimulating immunoglobulin, thyroid growth- stimulating immunoglobulin, TSH- binding inhibitor immunoglobulin Diffuse hypertrophy and hyperplasia with tall, crowded follicular cells
Thyroid Gland Diffuse nontoxic (simple) goiter- colloid goiter, iodine deficiency, clinically euthyroid, sporadic usually related to substances that interfere with thyroid hormone synthesis, mass effects from enlarging size Multinodular goiter- recurrent hyperplasia and involution from a long-standing simple goiter, mistaken for neoplasia, mass effects, occasionally toxic - hyperthyroidism
Thyroid gland Neoplasias Adenoma Carcinoma Papillary Follicular Anaplastic Medullary Congenital anomaly – Thyroglossal duct or cyst