Download
1 / 1
10 likes | 179 Views
A NEW EPIDEMIC: CHRONIC KIDNEY DISEASE IN GENERAL POPULATION REAL PREVALENCE AND RELATED FACTORS Josep M. Galceran, Rosa Garcia Osuna, Xavier Fulladosa, Josep M. Lisbona*, Jordi Coderch*. Nephrology and Information&Research* Departments. Hospital de Palamós, Catalunya, Spain. AIM.

E N D
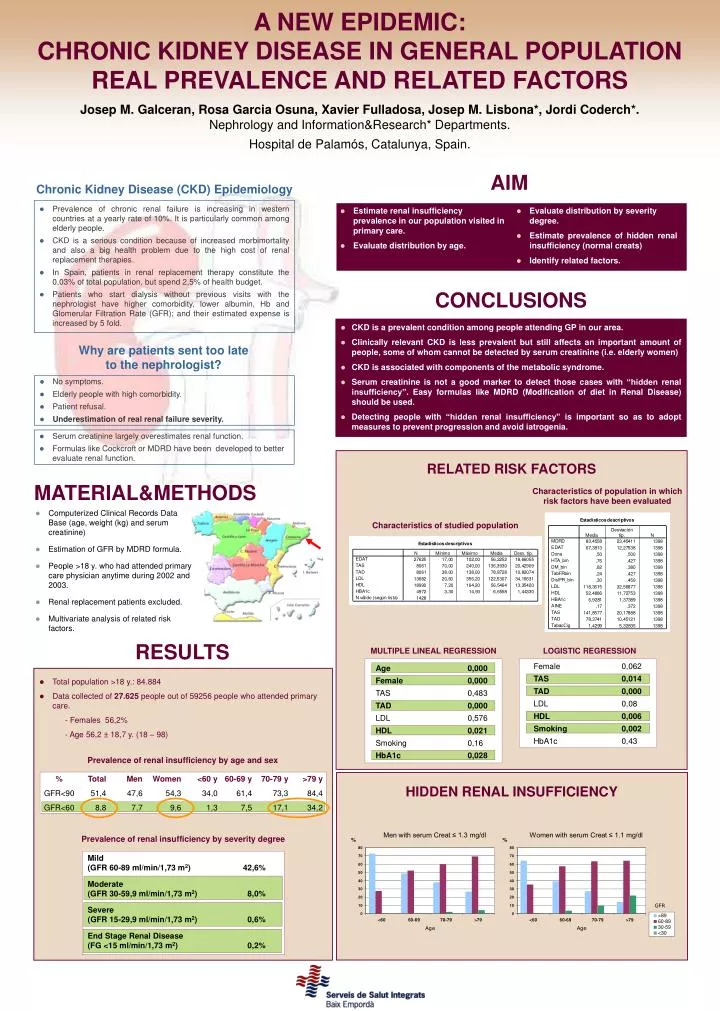
A NEW EPIDEMIC: CHRONIC KIDNEY DISEASE IN GENERAL POPULATION REAL PREVALENCE AND RELATED FACTORS Josep M. Galceran, Rosa Garcia Osuna, Xavier Fulladosa, Josep M. Lisbona*, Jordi Coderch*. Nephrology and Information&Research* Departments. Hospital de Palamós, Catalunya, Spain. AIM Chronic Kidney Disease (CKD) Epidemiology • Prevalence of chronic renal failure is increasing in western countries at a yearly rate of 10%. It is particularly common among elderly people. • CKD is a serious condition because of increased morbimortality and also a big health problem due to the high cost of renal replacement therapies. • In Spain, patients in renal replacement therapy constitute the 0,03% of total population, but spend 2,5% of health budget. • Patients who start dialysis without previous visits with the nephrologist have higher comorbidity, lower albumin, Hb and Glomerular Filtration Rate (GFR); and their estimated expense is increased by 5 fold. • Evaluate distribution by severity degree. • Estimate prevalence of hidden renal insufficiency (normal creats) • Identify related factors. • Estimate renal insufficiency prevalence in our population visited in primary care. • Evaluate distribution by age. CONCLUSIONS • CKD is a prevalent condition among people attending GP in our area. • Clinically relevant CKD is less prevalent but still affects an important amount of people, some of whom cannot be detected by serum creatinine (i.e. elderly women) • CKD is associated with components of the metabolic syndrome. • Serum creatinine is not a good marker to detect those cases with “hidden renal insufficiency”. Easy formulas like MDRD (Modification of diet in Renal Disease) should be used. • Detecting people with “hidden renal insufficiency” is important so as to adopt measures to prevent progression and avoid iatrogenia. Why are patients sent too late to the nephrologist? • No symptoms. • Elderly people with high comorbidity. • Patient refusal. • Underestimation of real renal failure severity. • Serum creatinine largely overestimates renal function. • Formulas like Cockcroft or MDRD have been developed to better evaluate renal function. RELATED RISK FACTORS MATERIAL&METHODS Characteristics of population in which risk factors have been evaluated • Computerized Clinical Records Data Base (age, weight (kg) and serum creatinine) • Estimation of GFR by MDRD formula. • People >18 y. who had attended primary care physician anytime during 2002 and 2003. • Renal replacement patients excluded. • Multivariate analysis of related risk factors. Characteristics of studied population RESULTS MULTIPLE LINEAL REGRESSION Age 0,000 Female 0,000 TAS 0,483 TAD 0,000 LDL 0,576 HDL 0,021 Smoking 0,16 HbA1c 0,028 LOGISTIC REGRESSION Female 0,062 TAS 0,014 TAD 0,000 LDL 0,08 HDL 0,006 Smoking 0,002 HbA1c 0,43 • Total population >18 y.: 84.884 • Data collected of 27.625 people out of 59256 people who attended primary care. - Females 56,2% - Age 56,2 ±18,7 y. (18 – 98) Prevalence of renal insufficiency by age and sex % Total Men Women <60 y 60-69 y 70-79 y >79 y GFR<90 51,4 47,6 54,3 34,0 61,4 73,3 84,4 GFR<60 8,8 7,7 9,6 1,3 7,5 17,1 34,2 HIDDEN RENAL INSUFFICIENCY Prevalence of renal insufficiency by severity degree Mild (GFR 60-89 ml/min/1,73 m2) 42,6% Moderate (GFR 30-59,9 ml/min/1,73 m2) 8,0% Severe (GFR 15-29,9 ml/min/1,73 m2) 0,6% End Stage Renal Disease (FG <15 ml/min/1,73 m2) 0,2%