Download
1 / 64
730 likes | 1.16k Views
Antibody-Mediated Rejection in Renal transplantation.

E N D
Homo transplants differ not only in the strength of rejection, but also in the nature and location of the phenomena induced by rejection. This conclusion must not be regarded as a cause for discouragement. On the contrary, it should spur further research. —Jean Hamburger
Antibody-mediated rejection • Alloantibodies are now appreciated as important mediators of acute and chronic rejection • Alloantibodies to HLA class I or II and other antigens expressed by endothelium cause a variety of effects on renal transplants, ranging from acute to chronic rejection, and even apparent graft acceptance (accommodation). • It differs in pathogenesis, or “nature,” from T cell–mediated rejection.
Antibody-mediated rejection • Alloantibodies preferentially attack a different “location,” namely • the peritubular and glomerular capillaries, in contrast to T cells, which characteristically infiltrate tubules and arterial endothelium. • Antibody-mediated rejection generally has a worse prognosis and requires a different form of therapy than the usual T cell–mediated acute rejection
Antibody-mediated rejection and C4d • C4d is a fragment of C4b, an activation product of the classic complement pathway • C4d remains covalently bound in the tissue for several days after complement activation • C4d deposition is strongly associated with circulating antibody to donor HLA class I or class II antigens • C4d is currently the best single marker of complement-fixing circulating antibodies to the endothelium. Feucht et al Kidney Int 1993; 43:1333–1338. Mauiyyedi S et al. J Am Soc Nephrol 2002 ; 13: 779–787. Bohmig GA et al. J Am Soc Nephrol 2002; 13: 1091–1099
Complement activation pathways. The classic pathway is relevant to antibody-mediated rejection
Antibody-mediated rejection • Four forms of antibody-mediated graft injury have been defined • Hyperacute rejection • Acute humoral rejection • Chronic humoral rejection • Accommodation
Stages of Antibody Mediated rejection • Stages I to II represent accommodation, stage III represents subclinical humoral rejection, and stage IV represents CHR. • The dashed lines for antibody and C4d deposition are meant to reflect the possibility of intermittent positivity over time. • Inevitability of progression is not meant to be implied by the term “stages.” The rate of progression is likely to be variable, and the early stages, I and II, are reversible. At any stage, the antibody/ C4d may become negative, in which case the process is inactive. Colvin RB. J Am Soc Nephrol 18: 1046–1056, 2007
Definition Hyperacute rejection • Hyperacute rejection arises within minutes or hours in presensitized patients who have circulating HLA, ABO, or other alloantibody-to-donor endothelial surface antigens
Hyperacute Rejection • The pathology of hyperacute rejection overlaps completely with AHR. • Deposition of C4d occurs in PTC and glomeruli, just as in AHR • Early biopsies may be negative for C4d, presumably because of lack of access of C4 to the site (vasoconstriction) or enough time for sufficient amount to be deposited.
Hyperacute rejection • Mediated by Rapid thrombotic occlusion of the vasculature of the transplanted allograft • Occurs within minutes to hours after host blood vessels are anastomosed to donor vessels • Mediated predominantly by IgG antibodies directed toward foreign protein molecules, such as MHC molecules • Result from prior exposure to alloantigens from blood transfusions, pregnancy, or previous transplantation
Acute humoral rejection • Definition • Rapid loss of graft function (days), any time after transplantation • An acute loss of graft function that often arises in the first few weeks after transplantation • Cannot be distinguished from cell-mediated rejection on clinical grounds
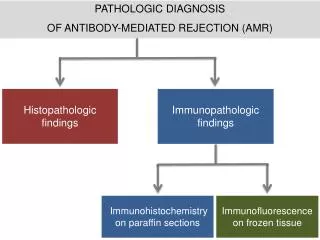
Acute humoral rejection • Antibody-mediated rejection frequently undiagnosed • Lack of typical morphologic characteristics • C4d immunohistochemistry • C4 is an element of the complement cascade • Its degradation product (C4d) adheres to endothelial cells • Can be detected by pathologist
Acute humoral rejection • Classification of rejection as either “cellular” or “humoral” is flawed • Significant overlap exists 1 Montgomery R, Zachary AA. Transplantation 2000;70:887–894, 2 Becker YT et al , Am J Transplant 2004;4:996-1001
Diagnostic criteria for acute antibody-mediated rejection (AHR) • Morphologic evidence of acute tissue injury acute tubular injury • neutrophils and/or mononuclear cells in PTC and/or glomeruli and/or capillary thrombosis fibrinoid necrosis/intramural or transmural inflammation in arteries • Immunopathologic evidence for antibody action C4d and/or (rarely) immunoglobulin in PTC Ig and complement in arterial fibrinoid necrosis • Serologic evidence of circulating antibodies to donor HLA or other anti-donor endothelial antigen Cases that meet only two of the three numbered criteria are considered suspicious for AHR. Acute cellular rejection may also be present. Colvin RB. J Am Soc Nephrol 18: 1046–1056, 2007
Patterns of Rejection in ABO Incompatible Transplants AMR Cellular Accommodation
Therapeutic Options For The Treatment Of AMR Antibody Reduction Immunomodulation • Plasmapheresis/IA • IVIg • IVIg • ATG • IL-2R blockers • Fk 506, Rapamycin • MMF/DSG • CAMPATH? B-cell Modulation • Splenectomy • Anti-CD20 • Cytoxan
Antibody Reduction Therapy • High dose IVIG (1-2 gms/kg) • Mechanism: • Anti-idiotypic networks probably important • Many putative immunomodulatory pathways identified • Advantages: • In vitro test for predicting efficacy • Ease of administration? • Disadvantages: • Non-responders • Different techniques required to follow DSA titers • Less rapid Ab removal, unproven for high-titer DSA • Toxicity & batch-to-batch variability • Unproven for ABOi Tx
Antibody Reduction Therapy • Plasmapheresis/Low Dose IVIg (100 mg/kg) • Mechanism: • Rapid reduction in anti-HLA or isoagglutinin Ab • Induces donor specific unresponsiveness (HLA) or accommodation (ABOI) • Advantages: • Predictable kinetics of plasmapheresis • No evidence of “nonresponders” • Able to easily follow DSA levels during/after therapy • Disadvantages: • DSA may rebound between treatments or if discontinued • Treatment may be prolonged and immunosuppressive • Expensive and resource intensive
Rituximab • Monoclonal anti-CD20 antibody (found on B cells) • May improve outcomes in antibodymediated acute rejection episodes 1 Montgomery R, Zachary AA. Transplantation 2000;70:887–894, 2 Becker YT et al , Am J Transplant 2004;4:996-1001
B-Cell Modulation • Anti-CD20 • Mechanism: • Rapid ablation of the peripheral B-cell compartment • Advantages: • Probably reduces precursor cells responsible for clonal expansion during AMR • May produce more effective antibody reduction when combined with plasmapheresis or IVIG • Well-tolerated, little apparent toxicity • Effect on the immune system is temporary (6-months) • Disadvantages: • Plasma cells persist in the spleen • May not, on its own, reduce DSA titers during AMR • Immunosuppressive
Case Study: AMR in (+) Cytotoxic XM with High Titer Anti-HLA DSA DSA titer Cr 6.5 512 PP/ CMVIg PRA 128 100 Cr 4.4 100 100 100 98 120 90 Cr 2.1 Cr 1.5 Cr 1.6 80 85 100 70 DSA titer 80 PRA 60 58 64 50 60 Anti-CD20 CD20=0 CD19=0 CD20=23.7 40 40 30 32 32 Tx 20 16 16 16 16 16 20 8 8 8 8 8 8 10 4 4 4 4 4 2 2 2 1 1 1 0 0 0 -19 -17 -15 -12 -8 -7 -6 -5 -4 -3 -2 -1 0 +2 +3 +4 +5 +6 +7 +8 +9 +11 +12 +13 +16 +18 +19 Days from Transplant
B-cell Modulation • Splenectomy • Mechanism: • Reduces plasma cells, precursor cells, B-cell immune surveillance capabilities • Advantages: • Can be performed using minimally invasive techniques • May produce more effective antibody reduction when combined with plasmapheresis or IVIG • Disadvantages: • Life-long risk of sepsis from encapsulated bacteria • Does not appear on its own to reduce DSA titers • Effect on immune system is permanent
The Effect of Splenectomy on Anti-Blood Group Ab PP/IVIg 512 256 4 Splenectomy 3 Anti-A Titers (1:X) Serum Creatinine (mg/dL) 128 Tx 2 64 1 32 16 0 -28 -23 -21 -18 -16-15 -14 -12 -10 -6 -4 -3 -2 -1 0 3 5 7 8 10 12 14 17 21 25 27 31 32 34 40 42 45 Day With Respect to Transplant
Targets of Strategies for Antibody Removal Plasmapheresis/IVIG Plasma cells Splenectomy Clonal Expansion B-cells & Pre B-cells Anti-CD20
Acute De Novo AMR • Occurs in 4-6% of transplants (80-100% fail) • By definition the current XM is negative • Risk factors include: + historic XM, • history of sensitizing event(s), high risk • donor/recipient combination • Historically suspected only after there is a poor • response to anti-lymphocytic agents • Diagnosis should be made by histology and • demonstration of the appearance of DSA
PP/CMVIg Treatment Protocolfor Acute De Novo AMR Plasmapheresis – single plasma volume exchange Steroid bolus -OR- a-thymocyte globulin IVIG – 100mg/kg following each PP treatment (CMV hyperimmune globulin) PP/Ig PP/Ig PP/Ig PP/Ig PP/Ig Dx of AMR 2 4 6 8 Time Relative to Initiation of Therapy (Days) Heparin D/C FK 506 High Grade: Johns Hopkins InKTP
15 * * * 10 Serum Creatinine (mg/dL) 5 0 Nadir Rejection 1 Week 1 Month Current De Novo AMR: Renal Allograft Function * p<0.001 1994-2003: 22 recipients of deceased or live donor kidney transplants with AMR by Bx or DSA treated with PP/IVIg Mean f/u: 5 1/2 years Johns Hopkins InKTP
100 90 80 70 60 50 40 30 20 10 0 365 730 1095 Time (days) Live donor Deceased donor PP/CMVIg Treatment for De Novo AMR 100 100 Allograft Survival 90 90 80 80 70 70 LiveDeceased p = NS 60 60 p = NS 50 50 1-Year: 87.5% 85.8% 40 40 30 30 20 20 3-Year: 87.5% 77.1% 10 10 0 0 365 365 730 730 1095 1095 Time (days) Time (days) 5-Year: Overall 81.1% Live donor Deceased donor Live donor Deceased donor Kaplan-Meier Estimate of Graft Survival for recipients who developed de novo AMR and were treated with PP/CMVIg therapy Johns Hopkins InKTP
Bx and DSA Proven De Novo AMR Johns Hopkins InKTP
De Novo Renal Function 15 12 9 Serum Creatinine (mg/dL) 6 3 0 LD DD Creatinine at Biopsy Creatinine 1 week Creatinine 1 mo Current Cr P=NS for comparison between groups at each timepoint Johns Hopkins InKTP
De Novo AMR Allograft Survival 100.00 90.00 80.00 70.00 60.00 Survival (%) 50.00 40.00 30.00 20.00 10.00 0.00 0 6 12 18 24 30 36 Time (Months) Live Deceased Johns Hopkins InKTP
Rejection and Clinical Outcomes Following(+) XM and ABOi ABO INCOMPATIBLE POSITIVE CROSSMATCH # OF PATIENTS 28 # OF PATIENTS 86 1 2 3 4 1 0 1 2 3 31 12 5 Previous Txs Previous Txs 27/86 (31%) 26/86 (30%) AMR CELLULAR REJECTION AMR CELLULAR REJECTION 3/28 (11%) 4/28 (14%) 7/86 (8%)* 16/86 (19%) 0/28 (0%) 7/28 (25%) SUBCLINICAL AMR SUBCLINICAL CELLULAR SUBCLINICAL AMR SUBCLINICAL CELLULAR 89.8% 80.9% 1-YEAR GRAFT SURVIVAL 3-YEAR GRAFT SURVIVAL 92.9%** 92.9% 1-YEAR GRAFT SURVIVAL 3-YEAR GRAFT SURVIVAL **1 death WNE 1 Noncompliance *Bx @ 1, 3, 6, 12 mos Johns Hopkins InKTP
(+) XM vs. De Novo AMR Johns Hopkins InKTP
15 12 9 Serum Creatinine (mg/dL) 6 3 0 PP/CMVIg Desensitized De Novo Rejection Creatinine at Biopsy Creatinine 1 week Creatinine 1 mo Current Cr (+) XM vs. De Novo AMR Outcomes P=0.04 P=0.01 P=0.002 P=NS between groups at current timepoint Johns Hopkins InKTP
Allograft Survival After AMR (+) XM vs. De Novo 100.00 90.00 80.00 70.00 p=NS 60.00 Survival (%) 50.00 40.00 30.00 20.00 10.00 0.00 0 6 12 18 24 30 36 Time (Months) (+) XM DeNovo Johns Hopkins InKTP
100 90 80 70 60 % Allograft 50 Survival 40 30 20 10 0 30 60 90 120 150 180 210 240 270 300 330 360 Time (Days) + XM @ Tx - XM @ Tx Kaplan-Meier Estimate of Graft Survival (+) CDC XM @ Time of Tx vs (-) CDC XM 1 Year Graft Survival p=NS +XM @ Tx- XM @ Tx N= 14 N= 32 92.3% 87.2% Johns Hopkins InKTP
Anti-CD20 Rescue Protocol Inclusion Characteristics • Failure to Respond to Plasmapheresis/CMVIg Therapy • Poor or Incomplete Clinical Response • Persistence of High-Titer DSA • Persistence of Histologic Evidence of AMR • Initial Histologic Features That Portend Poor Outcome • and/or Graft Loss (Grade 2-3 AMR) • Study Group • Recipients of Deceased or Live Donor Kidneys • De novo AMR • AMR After Desensitization Johns Hopkins InKTP
Renal Function Following Anti-CD20 Rescue p=0.0003 p=0.01 10 p=0.07 9 p=0.25 8 7 17 recipients undergoing a-CD20 rescue therapy for AMR 6 5 4 3 2 1 0 2 weeks Current Best AMR 1 Month Best Cr AMR Cr 2 week Cr 1 month Cr Current Cr
Kaplan-Meier Estimate of Graft Survival for Anti-CD20 Rescue 100 75 % Survival 50 25 0 1 2 3 4 5 6 7 8 9 10 11 12 Months Following Anti-CD20 Treatment Johns Hopkins InKTP
Splenectomy Rescue Johns Hopkins InKTP
Paired Donation May Reduce the Incidence of AMR Conventional KPD Unconventional KPD ABOi ABOi A B A O (+) XM ABOi B A O A # of KPD: 6 (12 patients) # of KPD: 5 (13 patients) Mean PRA: 14 Mean PRA: 58 6 mos Cr: 1.2 mg/dl 6 mos Cr: 1.1 mg/dl Cellular 8% AMR: 0% Cellular 23% AMR: 0% Patient Survival: 100% Patient Survival: 100% Graft Survival: 91.7% Graft Survival: 100%
Other Therapies • Leflunomide • An orally administered antimetabolite • Action against NF-B and JAK3, key mediators in cytokine generation • Inhibits CMV • FTY720 • Reduces peripheral lymphocyte levels by causing sequestration in lymph nodes and Peyer patches • Efalizumab • Monoclonal anti-CD11a antibody • Blocks T cell adhesion • Alemtuzumab (Campath 1H) • Monoclonal antibody targeting CD52 (found on all lymphocytes) • Causes profound, prolonged lymphocyte depletion • Tolerance induction with full immunosuppression and bone marrow transplant
The diagnosis of AMR can now be made with a high level of certainty • There are therapeutic interventions for AMR with clinically proven efficacy • De novo AMR has a good long-term prognosis when treated with PP or IVIg • Results of PP or IVIg treatment for De novo AMR and AMR in the setting • of desensitization are comparable • A (+) cytotoxic XM at the time of Tx does not predict a worse outcome • AMR recalcitrant to PP/IVIg is associated with a lower graft survival rate • Results of emergent splenectomy at the time of severe AMR look promising • KPD may decrease AMR by lowering immunologic risk Summary
Algorithm For Approach To AMR De Novo AMR AMR after ABOi AMR after (+) XM PP/IVIg Response Severe AMR Incomplete Response Anti-CD20 Observe Anti-CD20 Splenectomy
Chronic antibody-mediated rejection
Definition Chronic antibody-mediated rejection (CHR) • Slow, progressive loss of graft function (months to years), often with proteinuria, hypertension Colvin RB. J Am Soc Nephrol 18: 1046–1056, 2007
Chronic rejection • Fibrosis and scarring in transplanted organ • Multifactorial etiology, not strictly immunologic • Inflammation, ischemia, and other processes play a role • Episodes of acute rejection are significant risk factors