Download
1 / 31
320 likes | 342 Views
Explore diagnostic criteria, treatment options, and case studies related to acute antibody-mediated rejection in organ transplantation. Learn about antibody reduction therapies, B-cell modulation, and the impact of splenectomy on immune responses.

E N D
Experience with Antibody-Mediated Rejection Millie Samaniego, M.D. Associate Professor of Medicine University of Wisconsin and Robert A. Montgomery, M.D., D.Phil. Chief, Division of Transplantation Director, The Johns Hopkins Comprehensive Transplant Center The Johns Hopkins Hospital
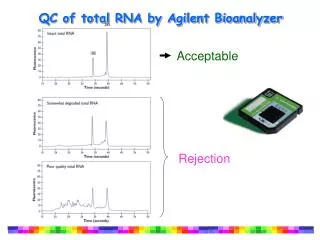
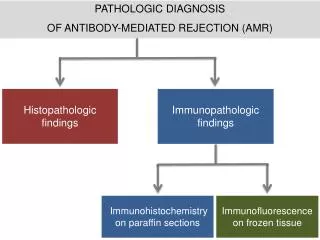
Diagnostic Criteria for Acute AMR • Characteristic histologic features including: • 1) glomerulitis/capillaritis • 2) margination of neutrophils in the PTC • 3) fibrin thrombi • 4) interstitial hemorrhage • 5) severe or necrotizing vasculitis • Diffuse, linear C4d staining in the PTC • Identification of DSA Grade 1 Grade 3
Patterns of Rejection in ABO Incompatible Transplants AMR Cellular Accommodation
Therapeutic Options For The Treatment Of AMR Antibody Reduction Immunomodulation • Plasmapheresis/IA • IVIg • IVIg • ATG • IL-2R blockers • Fk 506, Rapamycin • MMF/DSG • CAMPATH? B-cell Modulation • Splenectomy • Anti-CD20 • Cytoxan
Antibody Reduction Therapy • High dose IVIG (1-2 gms/kg) • Mechanism: • Anti-idiotypic networks probably important • Many putative immunomodulatory pathways identified • Advantages: • In vitro test for predicting efficacy • Ease of administration? • Disadvantages: • Non-responders • Different techniques required to follow DSA titers • Less rapid Ab removal, unproven for high-titer DSA • Toxicity & batch-to-batch variability • Unproven for ABOi Tx
Antibody Reduction Therapy • Plasmapheresis/Low Dose IVIg (100 mg/kg) • Mechanism: • Rapid reduction in anti-HLA or isoagglutinin Ab • Induces donor specific unresponsiveness (HLA) or accommodation (ABOI) • Advantages: • Predictable kinetics of plasmapheresis • No evidence of “nonresponders” • Able to easily follow DSA levels during/after therapy • Disadvantages: • DSA may rebound between treatments or if discontinued • Treatment may be prolonged and immunosuppressive • Expensive and resource intensive
B-Cell Modulation • Anti-CD20 • Mechanism: • Rapid ablation of the peripheral B-cell compartment • Advantages: • Probably reduces precursor cells responsible for clonal expansion during AMR • May produce more effective antibody reduction when combined with plasmapheresis or IVIG • Well-tolerated, little apparent toxicity • Effect on the immune system is temporary (6-months) • Disadvantages: • Plasma cells persist in the spleen • May not, on its own, reduce DSA titers during AMR • Immunosuppressive
Case Study: AMR in (+) Cytotoxic XM with High Titer Anti-HLA DSA DSA titer Cr 6.5 512 PP/ CMVIg PRA 128 100 Cr 4.4 100 100 100 98 120 90 Cr 2.1 Cr 1.5 Cr 1.6 80 85 100 70 DSA titer 80 PRA 60 58 64 50 60 Anti-CD20 CD20=0 CD19=0 CD20=23.7 40 40 30 32 32 Tx 20 16 16 16 16 16 20 8 8 8 8 8 8 10 4 4 4 4 4 2 2 2 1 1 1 0 0 0 -19 -17 -15 -12 -8 -7 -6 -5 -4 -3 -2 -1 0 +2 +3 +4 +5 +6 +7 +8 +9 +11 +12 +13 +16 +18 +19 Days from Transplant
B-cell Modulation • Splenectomy • Mechanism: • Reduces plasma cells, precursor cells, B-cell immune surveillance capabilities • Advantages: • Can be performed using minimally invasive techniques • May produce more effective antibody reduction when combined with plasmapheresis or IVIG • Disadvantages: • Life-long risk of sepsis from encapsulated bacteria • Does not appear on its own to reduce DSA titers • Effect on immune system is permanent
The Effect of Splenectomy on Anti-Blood Group Ab PP/IVIg 512 256 4 Splenectomy 3 Anti-A Titers (1:X) Serum Creatinine (mg/dL) 128 Tx 2 64 1 32 16 0 -28 -23 -21 -18 -16-15 -14 -12 -10 -6 -4 -3 -2 -1 0 3 5 7 8 10 12 14 17 21 25 27 31 32 34 40 42 45 Day With Respect to Transplant
Targets of Strategies for Antibody Removal Plasmapheresis/IVIG Plasma cells Splenectomy Clonal Expansion B-cells & Pre B-cells Anti-CD20
Acute De Novo AMR • Occurs in 4-6% of transplants (80-100% fail) • By definition the current XM is negative • Risk factors include: + historic XM, • history of sensitizing event(s), high risk • donor/recipient combination • Historically suspected only after there is a poor • response to anti-lymphocytic agents • Diagnosis should be made by histology and • demonstration of the appearance of DSA
PP/CMVIg Treatment Protocolfor Acute De Novo AMR Plasmapheresis – single plasma volume exchange Steroid bolus -OR- a-thymocyte globulin IVIG – 100mg/kg following each PP treatment (CMV hyperimmune globulin) PP/Ig PP/Ig PP/Ig PP/Ig PP/Ig Dx of AMR 2 4 6 8 Time Relative to Initiation of Therapy (Days) Heparin D/C FK 506 High Grade:
15 * * * 10 Serum Creatinine (mg/dL) 5 0 Nadir Rejection 1 Week 1 Month Current De Novo AMR: Renal Allograft Function * p<0.001 1994-2003: 22 recipients of deceased or live donor kidney transplants with AMR by Bx or DSA treated with PP/IVIg Mean f/u: 5 1/2 years
100 90 80 70 60 50 40 30 20 10 0 365 730 1095 Time (days) Live donor Deceased donor PP/CMVIg Treatment for De Novo AMR 100 100 Allograft Survival 90 90 80 80 70 70 LiveDeceased p = NS 60 60 p = NS 50 50 1-Year: 87.5% 85.8% 40 40 30 30 20 20 3-Year: 87.5% 77.1% 10 10 0 0 365 365 730 730 1095 1095 Time (days) Time (days) 5-Year: Overall 81.1% Live donor Deceased donor Live donor Deceased donor Kaplan-Meier Estimate of Graft Survival for recipients who developed de novo AMR and were treated with PP/CMVIg therapy
De Novo Renal Function 15 12 9 Serum Creatinine (mg/dL) 6 3 0 LD DD Creatinine at Biopsy Creatinine 1 week Creatinine 1 mo Current Cr P=NS for comparison between groups at each timepoint
De Novo AMR Allograft Survival 100.00 90.00 80.00 70.00 60.00 Survival (%) 50.00 40.00 30.00 20.00 10.00 0.00 0 6 12 18 24 30 36 Time (Months) Live Deceased
Rejection and Clinical Outcomes Following(+) XM and ABOi ABO INCOMPATIBLE POSITIVE CROSSMATCH # OF PATIENTS 28 # OF PATIENTS 86 1 2 3 4 1 0 1 2 3 31 12 5 Previous Txs Previous Txs 27/86 (31%) 26/86 (30%) AMR CELLULAR REJECTION AMR CELLULAR REJECTION 3/28 (11%) 4/28 (14%) 7/86 (8%)* 16/86 (19%) 0/28 (0%) 7/28 (25%) SUBCLINICAL AMR SUBCLINICAL CELLULAR SUBCLINICAL AMR SUBCLINICAL CELLULAR 89.8% 80.9% 1-YEAR GRAFT SURVIVAL 3-YEAR GRAFT SURVIVAL 92.9%** 92.9% 1-YEAR GRAFT SURVIVAL 3-YEAR GRAFT SURVIVAL **1 death WNE 1 Noncompliance *Bx @ 1, 3, 6, 12 mos
15 12 9 Serum Creatinine (mg/dL) 6 3 0 PP/CMVIg Desensitized De Novo Rejection Creatinine at Biopsy Creatinine 1 week Creatinine 1 mo Current Cr (+) XM vs. De Novo AMR Outcomes P=0.04 P=0.01 P=0.002 P=NS between groups at current timepoint
Allograft Survival After AMR (+) XM vs. De Novo 100.00 90.00 80.00 70.00 p=NS 60.00 Survival (%) 50.00 40.00 30.00 20.00 10.00 0.00 0 6 12 18 24 30 36 Time (Months) (+) XM DeNovo
100 90 80 70 60 % Allograft 50 Survival 40 30 20 10 0 30 60 90 120 150 180 210 240 270 300 330 360 Time (Days) + XM @ Tx - XM @ Tx Kaplan-Meier Estimate of Graft Survival (+) CDC XM @ Time of Tx vs (-) CDC XM 1 Year Graft Survival p=NS +XM @ Tx- XM @ Tx N= 14 N= 32 92.3% 87.2%
Anti-CD20 Rescue Protocol Inclusion Characteristics • Failure to Respond to Plasmapheresis/CMVIg Therapy • Poor or Incomplete Clinical Response • Persistence of High-Titer DSA • Persistence of Histologic Evidence of AMR • Initial Histologic Features That Portend Poor Outcome • and/or Graft Loss (Grade 2-3 AMR) • Study Group • Recipients of Deceased or Live Donor Kidneys • De novo AMR • AMR After Desensitization
Renal Function Following Anti-CD20 Rescue p=0.0003 p=0.01 10 p=0.07 9 p=0.25 8 7 17 recipients undergoing a-CD20 rescue therapy for AMR 6 5 4 3 2 1 0 2 weeks Current Best AMR 1 Month Best Cr AMR Cr 2 week Cr 1 month Cr Current Cr
Kaplan-Meier Estimate of Graft Survival for Anti-CD20 Rescue 100 75 % Survival 50 25 0 1 2 3 4 5 6 7 8 9 10 11 12 Months Following Anti-CD20 Treatment
Paired Donation May Reduce the Incidence of AMR Conventional KPD Unconventional KPD ABOi ABOi A B A O (+) XM ABOi B A O A # of KPD: 6 (12 patients) # of KPD: 5 (13 patients) Mean PRA: 14 Mean PRA: 58 6 mos Cr: 1.2 mg/dl 6 mos Cr: 1.1 mg/dl Cellular 8% AMR: 0% Cellular 23% AMR: 0% Patient Survival: 100% Patient Survival: 100% Graft Survival: 91.7% Graft Survival: 100%
Summary • The diagnosis of AMR can now be made with a high level of certainty • There are therapeutic interventions for AMR with clinically proven efficacy • De novo AMR has a good long-term prognosis when treated with PP or IVIg • Results of PP or IVIg treatment for De novo AMR and AMR in the setting • of desensitization are comparable • A (+) cytotoxic XM at the time of Tx does not predict a worse outcome • AMR recalcitrant to PP/IVIg is associated with a lower graft survival rate • Results of emergent splenectomy at the time of severe AMR look promising • KPD may decrease AMR by lowering immunologic risk
Algorithm For Approach To AMR De Novo AMR AMR after ABOi AMR after (+) XM PP/IVIg Response Severe AMR Incomplete Response Anti-CD20 Observe Anti-CD20 Splenectomy
Matt Cooper Lorraine Racusen Mark Haas Karen King Andrea Zachary Susie Lefell Donna Lucas Julie Graziani Renato Vega Chris Sonnenday Dan Warren Chris Simpkins Janet Hiller Jennie Rickard Amie Swardson James Burdick Edward Kraus Hamid Rabb Richard Ugarte Brigitte Reeb Mary Jo Holechek Diane Lepley Dorry Segev Tomasz Kazlowski Acknowledgements Johns Hopkins InKTP Johns Hopkins InKTP Columbia Lloyd Ratner