Download
1 / 3
50 likes | 394 Views
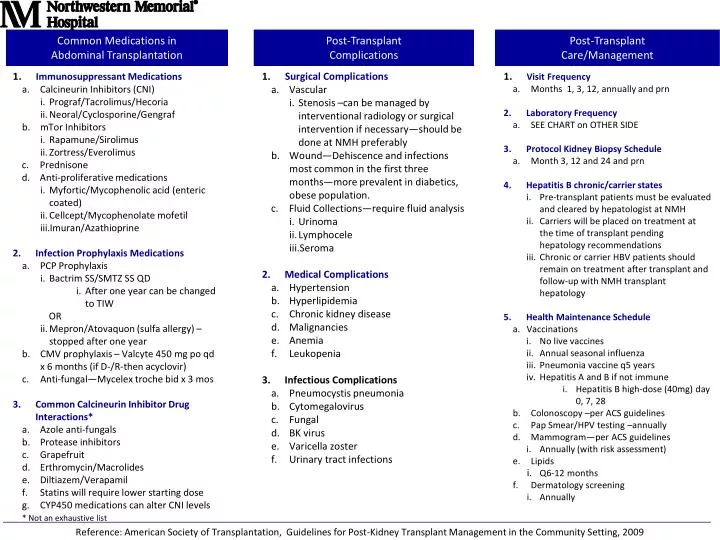
Common Medications in Abdominal Transplantation. Post-Transplant Complications. Post-Transplant Care/Management. 1. Visit Frequency Months 1 , 3 , 12, annually and prn Laboratory Frequency SEE CHART on OTHER SIDE Protocol Kidney Biopsy Schedule Month 3, 12 and 24 and prn

E N D
Common Medications in Abdominal Transplantation Post-Transplant Complications Post-Transplant Care/Management • 1. Visit Frequency • Months 1, 3, 12, annually and prn • Laboratory Frequency • SEE CHART on OTHER SIDE • Protocol Kidney Biopsy Schedule • Month 3, 12 and 24 and prn • Hepatitis B chronic/carrier states • Pre-transplant patients must be evaluated and cleared by hepatologist at NMH • Carriers will be placed on treatment at the time of transplant pending hepatology recommendations • Chronic or carrier HBV patients should remain on treatment after transplant and follow-up with NMH transplant hepatology • Health Maintenance Schedule • Vaccinations • No live vaccines • Annual seasonal influenza • Pneumonia vaccine q5 years • Hepatitis A and B if not immune • Hepatitis B high-dose (40mg) day 0, 7, 28 • Colonoscopy –per ACS guidelines • Pap Smear/HPV testing –annually • Mammogram—per ACS guidelines • Annually (with risk assessment) • Lipids • Q6-12 months • f. Dermatology screening • i. Annually • 1. Immunosuppressant Medications • Calcineurin Inhibitors (CNI) • Prograf/Tacrolimus/Hecoria • Neoral/Cyclosporine/Gengraf • b. mTor Inhibitors • Rapamune/Sirolimus • Zortress/Everolimus • Prednisone • Anti-proliferative medications • Myfortic/Mycophenolic acid (enteric coated) • Cellcept/Mycophenolatemofetil • Imuran/Azathioprine • Infection Prophylaxis Medications • PCP Prophylaxis • Bactrim SS/SMTZ SS QD • After one year can be changed to TIW • OR • ii. Mepron/Atovaquon (sulfa allergy) – stopped after one year • CMV prophylaxis – Valcyte 450 mg poqd x 6 months (if D-/R-then acyclovir) • Anti-fungal—Mycelex troche bid x 3 mos • Common Calcineurin Inhibitor Drug Interactions* • Azole anti-fungals • Protease inhibitors • Grapefruit • Erthromycin/Macrolides • Diltiazem/Verapamil • Statins will require lower starting dose • CYP450 medications can alter CNI levels • * Not an exhaustive list • 1. Surgical Complications • Vascular • Stenosis –can be managed by interventional radiology or surgical intervention if necessary—should be done at NMH preferably • b. Wound—Dehiscence and infections most common in the first three months—more prevalent in diabetics, obese population. • Fluid Collections—require fluid analysis • Urinoma • Lymphocele • Seroma • Medical Complications • Hypertension • Hyperlipidemia • Chronic kidney disease • Malignancies • Anemia • Leukopenia • Infectious Complications • Pneumocystis pneumonia • Cytomegalovirus • Fungal • BK virus • Varicella zoster • Urinary tract infections Reference: American Society of Transplantation, Guidelines for Post-Kidney Transplant Management in the Community Setting, 2009
Kidney, Kidney/Pancreas and Pancreas Alone Transplant Standard of Care (SOC) Labs Urine Dip to include: Protein, leukocytes, nitrites, protein, blood, glucose, blood; Reflex testing for Protein trace or >: order random urine protein and creatinine; Reflex testing for Leukocyte and/or nitrate positive: Order urine C&S +pancreas patients only; *only those child-bearing females (ages up to 60) on Myfortic, Cellcept, mycophenolatemofetil or mycophenolic acid; ^for patients who are HBsAg+ or HBcAb+
The Timeline of Post-Transplant Infections Modified from 1-3 Donor- Derived NOSOCOMIAL TECHNICAL DONOR/RECIPIENT Activation of Latent Infections, Relapsed, Residual, Opportunistic Infections COMMUNITY ACQUIRED TRANSPLANTATION DYNAMIC ASSESSMENT OF INFECTIOUS RISK Recipient- Derived < 4 WEEKS 1-6 MONTHS > 6 MONTHS Common Infections in Solid Organ Transplantation Recipients