Download
1 / 32
320 likes | 338 Views
This proposal aims to address the current issues in the adult heart allocation system, including high mortality rates for Status 1A candidates and inequitable geographic sharing. The goals of the proposal are to reduce waiting list mortality rates, reduce the use of exceptions for status qualification, and improve overall access to transplantation. The proposal introduces new urgency stratifications and modifies the geographic sharing scheme to ensure maximum utility of donor hearts. Implementation will require updating candidate data and verifying information. The proposal aligns with the OPTN Strategic Plan to improve equity in access to transplants.

E N D
Proposal to Modify the Adult Heart Allocation System Thoracic Organ Transplantation Committee Spring 2016
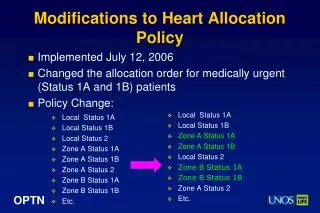
Current Allocation Policy Adult Candidate Prioritization: • Status 1A • Status 1B • Status 2 Zone C 1500 Miles Geographic Allocation Local: Status 1A, Status 1B Zone A: Status 1A, Status 1B Local: Status 2 Zone B: Status 1A, Status 1B Zone A: Status 2 Zone B: Status 2 Etc… Zone A 500 Miles Zone B 1000 Miles
What problems will the proposal solve? • Status 1A candidates are 3x more likely to die on the waiting list than candidates in any other status • High # of exception requests indicates certain candidates not served well by current system • Policy out of date re: increased use of mechanical circulatory support devices (MCSD) and associated complications • Current geographic sharing scheme is inequitable and inconsistent with the Final Rule
What are the goals of the proposal? • Reduce waiting list mortality rates amongst most urgent adult heart candidates • Reduce the use of exceptions to qualify for a status • Ensure qualifying criteria for statuses are based on objective physiological indications • Improve overall access to transplantation by modifying geographic distribution to ensure maximum utility of donor hearts
How does the proposal address the problem statement? • Adds more urgency stratifications based on relative waiting list mortality rates for all adult heart candidates • Modifies geographic sharing scheme to provide most urgent candidates access to donors from a broader geographic area
Proposed Statuses 4-6 *Candidates may qualify for more than one status, but their programs should register them in the most urgent status for which they qualify **Transplant programs can request exceptions to register candidates in statuses 1-4 if they don’t qualify based on policy but are as urgent as other candidates in those statuses
Waitlist mortality rates by simulation and new status groups, adult candidates Current Rules 6 Status 6 Status + Share Current Rules 6 Status 6 Status + Share Current Rules 6 Status 6 Status + Share Current Rules 6 Status 6 Status + Share Current Rules 6 Status 6 Status + Share Current Rules 6 Status 6 Status + Share 6 Statuses Current Rules 6 Status + Share 2 3 5 6 4 Inactive Simulation results show a range of outcomes across the ten runs, as well as a point estimate of the average across the runs. The ranges do not indicate confidence limits.
Transplant rates by simulation and new status groups, adult candidates 6 Statuses 6 Statuses 6 Statuses 6 Statuses 6 Statuses 6 Statuses Current Rules Current Rules Current Rules Current Rules Current Rules Current Rules 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share Simulation results show a range of outcomes across the ten runs, as well as a point estimate of the average across the runs. The ranges do not indicate confidence limits.
Two-year post-transplant mortality rates by simulation and tier, adult recipients 6 Statuses 6 Statuses 6 Statuses 6 Statuses 6 Statuses 6 Statuses Current Rules Current Rules Current Rules Current Rules Current Rules Current Rules 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share 6 Status + Share Simulation results show a range of outcomes across the ten runs, as well as a point estimate of the average across the runs. The ranges do not indicate confidence limits.
Impact on Pediatric Candidates • No negative impact anticipated • Potential for positive impact on pediatric candidate access to transplant • Modeling results for 6 urgency statuses with broader sharing: • Increased transplant counts for pediatric candidates • Increased transplant rates for status 1A pediatric candidates • Overall death counts decrease slightly
How will members implement this proposal? • Update data for candidates registered at the time of implementation • UNOS will provide a window of time during which members can update data • Members will need to verify the information after implementation date • Submit candidate CPRA values at time of registration and removal • CPRA already collected at time of transplant
How does this proposal support the OPTN Strategic Plan? • Strategic Goal – Improve Equity in Access to Transplants • More equitable access to transplants based on medical urgency and on geographic location
Questions? Joe Rogers, MD Committee Chair Joseph.rogers@duke.edu Liz Robbins Callahan, Esq. Project Liaison Liz.robbins@unos.org
Heart Allocation Score • OPTN does not collect enough data to develop a score • Inflexible solution • Changes in heart transplant technology occurring too quickly
ECMO Priority • Will ECMO in highest priority incentivize increased use of ECMO? • If so, will post-transplant outcomes be worse? • Is there potential for outcomes to be better if ECMO patients are transplanted quicker?
Total Artificial Heart (TAH) • Proposal: all TAH candidates grouped together in status 2 (hospitalized and not hospitalized) • Debate about whether outpatient TAH are more stable (should they be in a lower status?) • Debate about whether inpatient TAH are less stable (should they be in a higher status?)
Sensitized Candidates • Committee considered: • How to prioritize sensitized heart candidates • Definition of sensitization for heart candidates • Problem: can’t define sensitization for heart candidates because of insufficient OPTN data • Solution: collect more data • CPRA for each candidate upon registration and removal
LVAD for 30 Days • Debate: • Eliminate 30 day time • Candidates are at lower risk of developing adverse events when using this criterion • Candidates using this criterion have lower WL mortality risk than others in same status • Retain 30 day time • Candidates shouldn’t have to risk becoming unstable to get priority for transplant • Proposal: retains elective 30 day time for stable LVAD patients in status 3 • Represents compromise because 30 day time is mitigated by: • the proposed sharing scheme • Limitations on use with multiple registrations
Adult Heart Allocation Proposal – Waiting Time Transition Plan
Transplant counts and posttransplant outcomes by simulation and zone