Download
1 / 8
90 likes | 486 Views
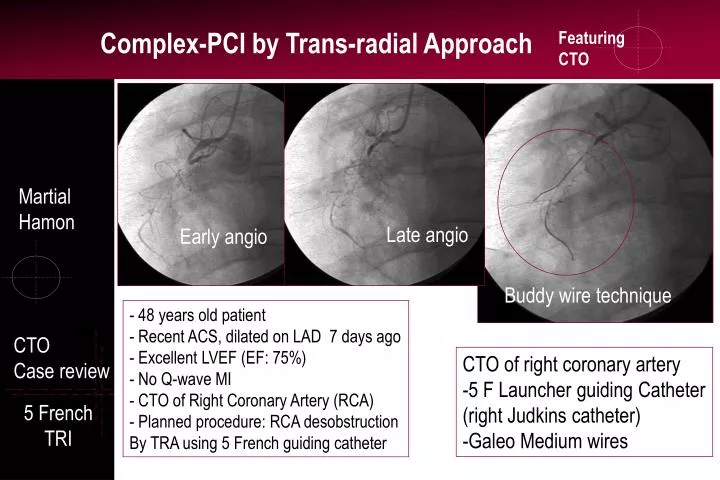
Martial Hamon. Late angio. Early angio. Buddy wire technique. 48 years old patient Recent ACS, dilated on LAD 7 days ago Excellent LVEF (EF: 75%) No Q-wave MI CTO of Right Coronary Artery (RCA) Planned procedure: RCA desobstruction By TRA using 5 French guiding catheter. CTO

E N D
Martial Hamon Late angio Early angio Buddy wire technique • 48 years old patient • Recent ACS, dilated on LAD 7 days ago • Excellent LVEF (EF: 75%) • No Q-wave MI • CTO of Right Coronary Artery (RCA) • Planned procedure: RCA desobstruction • By TRA using 5 French guiding catheter CTO Case review • CTO of right coronary artery • 5 F Launcher guiding Catheter • (right Judkins catheter) • -Galeo Medium wires 5 French TRI
Pathology of CTO Lesions FOCUS • Small vascular channels (160 to 230 microns diameter) • Connect with proximal part • Non visualized by angiography • Islands of dense fibrous tissues Background Pathology • Early angiogram frequently no entrance visible • Late angiogram distal opacification seen
Advanced PCI Patient : Potential Complications: • Documented ischemia? • Vessel importance? • Alternative solutions? • Optimal medications? • Benefit / risk? 1. Functional vs absolute occlusions 2. Duration of occlusion (>3months) 3. Morphology at occlusion point (tapered vs abrupt, bridging coll., side branch) 4. Lesion length AMI, CABG, death,perforation, tamponade, excessive contrast load and fluoroscopic Patient Selection Predictors of success : Lesion Selection
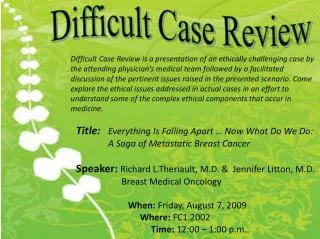
5 F provides optimal backupand support (deep cannulation was possible as seen in figures 2 and 3 by gentle clockwise rotation of the guiding catheter, Launcher 5F from Medtronic) Guide wire Galeo M was successful using buddy wire technique (Figure 1, Galeo M wire from Biotronik) Low-profile balloon: 1.25 mm in diameter and 15 mm length from Terumo was used to create the first channel (Figure 2, Riujyn balloon from Terumo) Fig.1 Fig.2 Fig.3 Buddy wire technique Low-profile balloon Long balloon dilation CTO 5 French TRI
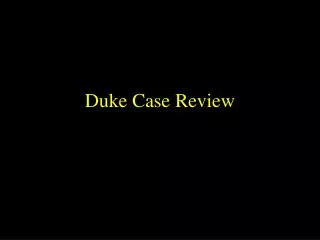
After balloon inflations After implantation of stents CTO CTO by trans-radial approach and with 5 French guiding catheter Is safe and feasibile in selected cases and with adapted materials 5 French TRI
1. Guiding catheters (optimal backup and support) 2. Guide wire support catheter (or over the wire balloon) 3. Guide wire (intermediate and stiffer, tapered and hydrophilic) 4. Interventional devices (low-profile balloons, rotablator, …) 5. Stents and DES (restenosis) 6. IVUS Material Selection Recommendations Hydrophilic guidewire Tapered-tip guidewire
Double guide wire technique (buddy wire) Side branch Vasa-vasorum Vasa vasorum Side branch Technichal aspects
Advanced PCI Advanced specific recommendations: • IVUS Guidance (entry site, complex dissection) • Contro-lateral access (dual arterial access sites) • Stiff wires (penetration wire) • Anchorage techniques • Rotablator (calcified lesion) • Meticulous review of angiograms+++ The last Frontier Key points