Download
1 / 22
220 likes | 342 Views
Overview of PAL strategy. Salah-Eddine Ottmani, MD, MPH TB Strategy and Operations Unit Stop TB Department WHO, Geneva Workshop on TB proposal preparation for Round 6 of the Global Fund to fight AIDS, TB and Malaria Geneva, 15 - 18 May 2006.

E N D
Overview of PAL strategy Salah-Eddine Ottmani, MD, MPH TB Strategy and Operations Unit Stop TB Department WHO, Geneva Workshop on TB proposal preparation for Round 6 of the Global Fund to fight AIDS, TB and Malaria Geneva, 15 - 18 May 2006
What is the rational behind the Practical Approach to Lung health (PAL) • Respiratory conditions are very common: 20 – 35% of patients in PHC setting • TB cases account for a very small proportion among respiratory patients • TB patients and the other respiratory patients have, in general, similar symptoms • In most countries, respiratory patients are managed, in PHC setting, on the basis of symptom presentation without clear systematic indications • A systematic, standardized and sound approach is needed to correctly identify TB cases among a huge number of respiratory patients
What is PAL strategy? • Syndromic management of patients who attend health services for respiratory symptoms • Focus on 1. PHC setting 2. Priority respiratory diseases > 5 yrs: + TB + ARI (pneumonia) + CRDs: mainly Asthma, COPD
What are the objectives of PAL strategy? PAL has 2 objectives: • 1. Improvement of the quality of care for every respiratory patient in PHC setting • 2. Improvement of the efficiency of health care delivery system for respiratory diseases in general
What are the components of PAL strategy? PAL has 2 components: • 1. Standardization of health care procedures: management and follow-up through the adaptation and development of clinical guideline • 2. Coordination among: • health care levels • the components of the health system particularly at district level
How to introduce PAL strategy in country? • Should be adapted to health environment of country • National health policy • Health priorities • Health resources • Country epidemiological profile • Should follow successive steps to be developed and implemented
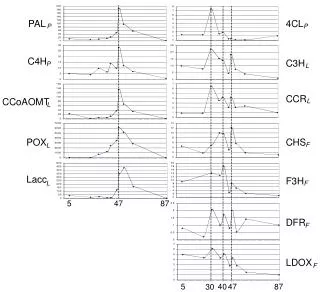
Distribution of respiratory diseases’ burden (in DALYs) in the population over 15 years of age by epidemiological profile and socioeconomic status
Countries with PAL activities (May 2006) • Countries at the preliminary phase: • Discussion: Costa-Rica, Mexico, Venezuela • Official request: China, Iran • Countries at the phase of adaptation and development: • Egypt, Lebanon, Lithuania, Oman, Rep. Korea (South) • Countries at the phase of feasibility test: • Algeria, Estonia, Guinea, Peru, Syria, Uganda • Countries at the preparatory phase of implementation: • Bolivia, Jordan and Tunisia • Countries at the phase of implementation: • Chile, El Salvador, Kyrgyzstan, Morocco, South Africa (FSP and WCP) • Operational research: Nepal
Key results from country experience • PAL is likely to decrease the referral of respiratory patients to upper health level; this suggests that PAL is liklely to improve the integration in PHC (Kyrgyzstan, Jordan, Bolivia) • PAL is likely to improve the quality of the process of diagnosis of TB (South-Africa, Tunisia, Bolivia??) • PAL is likely to improve TB case detection among respiratory patients in PHC (adj. OR=1.72, in South Africa) • PAL decreases drug prescription, particularly antibiotics and adjuvant drugs (Bolivia, Jordan, Kyrgyzstan, Morocco, Nepal, Tunisia) • PAL improves the quality drug prescription for CRD patients (Chile, Jordan, Kyrgyzstan, Morocco, South Africa, Tunisia) • PAL reduces the average cost of drug prescription per respiratory patient (Bolivia, Jordan, Kyrgyzstan, Morocco, Tunisia)
Impact on the referral of respiratory patients in Kyrgyzstan Referral Baseline study Impact study Variation p-value No (%) No (%) in % 893 (100.0) 992 (100.0) ----------------------------------------------------------------------------------------------- Overall referral 358 (40.1) 266 (26.8) - 33.2 < 0.0001 Hospital 17 (1.9) 7 (0.7) - 63.2 < 0.03 Specialists 102 (11.4) 52 (5.2) - 54.4 < 0.0001 Ancillary tests 321 (35.9) 241 (24.9) - 30.6 < 0.0001 Laboratory tests 245 (27.4) 185 (18.6) - 32.1 < 0.0001 Chest x-ray 171 (19.1) 114 (11.5) - 39.8 < 0.0001 ----------------------------------------------------------------------------------------------
Impact on the overall referral of respiratory patients in Bolivia, Jordan and Kyrgyzstan Referral Baseline study Impact study Variation p-value in % ----------------------------------------------------------------------------------------------- Bolivia 137/1033 (13.3%) 100/1154 (8.7%) - 34.6 < 0.001 Jordan 386/6287 (6.1%) 121/2719 (4.5%) - 26.2 < 0.01 Kyrgyzstan 358/893 (40.1%) 266/992 (26.8%) - 33.2% < 0.0001 Tunisia 134/2366 (5.7%) 172/1475 (11.7%) + 101.0% < 0.0001 -----------------------------------------------------------------------------------------------
SSE request among patients with respiratory symptoms for more than 2 weeks, Tunisia Type of study SSE request Total Proportion RP --------------------------------------------------------------------------- Baseline 8 160 5.0% 1 Impact 23 129 17.8% 3.6 X2= 12.28, p < 0.001 --------------------------------------------------------------------------- Total 31 289 10.7% --------------------------------------------------------------------------- SSE: sputum smear examination; TB: tuberculosis; RP: ratio of proportions.
SSE request among patients with respiratory symptoms for less and more than 2 weeks, Bolivia Type of study SSE request Total Proportion RP p-value --------------------------------------------------------------------------------------- Baseline ≥ 15 days 48 113 42.5% 6.1 < 0.0001 15 days <43 920 4.7% 1 Impact ≥ 15 days 54 98 55.1% 42.4 < 0.0001 15 days <14 1055 1.3% 1 ---------------------------------------------------------------------------------------- Total 159 2186 7.3%
Controlled trial, Free State Province, South Africa TBNon TBRP adj.OR ------------------------------------------------------------------ PAL 57 873 1.67 1.72 (p = 0.01) (p = 0.04) No PAL 34 892 1 1 ------------------------------------------------------------------ Total 91 1765
PAL impact on drug prescription in five countries Morocco Kygyzstan Tunisia Jordan Bolivia ---------------------------------------------------------------------------------------------------------- % patients with drug prescription - 3.1%*+ 2.6%** - 2.5%* 0.0% + 0.1%§ Ratio of drugs per patients who received drug prescription - 15%*- 11.1%* - 18.8%* - 12.2%* - 16.2%* % patients with ATB among all respi. patients - 25%*- 22.0%* - 21.1%* - 15.9%* - 11.1%** Average drug prescription cost per patient - 18%*- 32.4%* -19.3%* - 8.7%*** - 32.2%* ---------------------------------------------------------------------------------------------------------- *: p<0.001, **: p < 0.01, ***: p < 0.05, §: p > 0.05.
Variations in prescription frequencies of the adjuvant drugs after training in PAL among patients who received any drug prescription Bolivia Jordan Kyrgyzstan Tunisia ---------------------------------------------------------------------------------------------------------- Expectorant - 88.9% - 37.3% - 17.2% - 47.3% Vitamin - 57.1% - 100.0% - 41.7% - 14.7% NSAID + 163.3% - 41.7% - 28.8% Aspirin - 50.0% + 375.0% - 49.4% - 33.1% Antitussive - 47.0% - 19.8% - 2.0% Nasal decongestant + 4.5% + 75.0% + 26.8% + 0.4% Paracetamol - 43.8% - 4.3% + 62.7% + 17.8% Antihistaminic - 79.3% - 45.4% - 51.3% Average cost per patient - 25.1% - 16.3% - 30.9% - 20.2%
PAL impact on bronchodilator prescription, Kyrgyzstan • Among patients who received a drug prescription: • Reduction by 35.1% (baseline: 94/850; impact: 70/969) • Among patients who received bronchodilator prescription: • 26.6% increase of beta-2-agonist prescription (baseline: 53/94; impact: 50/70) • 26.5% increase of the average cost per patient (baseline: 155.0 Coms; impact: 196.0 Coms)
Bronchodilator prescription, Tunisia Bronchodilator Baseline Impact Variation p-value drug study study in % No = 2341 No = 1422 ---------------------------------------------------------------------------------------- Any bronchodilator 4.7% 5.8% + 23.4 0.141 * Inhaled β agonist 2.2% 4.7% + 113.0 < 0.0001 * Other β agonist form 0.5% 0.1% - 80.0 0.07 * Theophylline 2.6% 2.3% - 11.5 0.547 *Other Bronchodilator 0.3% 0.0% - 100.0 0.530* ---------------------------------------------------------------------------------------- Among patients who were prescribed bronchodilator Inhaled β agonist 46.8% 80.7% + 72.4% < 0.0001 Average cost per patient 4.3 DT 2.7 DT - 36.4% < 0.03
PAL impact on corticosteroid prescription, Kyrgyzstan • Among patients who received a drug prescription: • Reduction by 54.3% (baseline: 39/850; impact: 20/969) • Among patients who received corticosteroid prescription: • Inhaled steroid prescription 4.3 times more in the impact study (baseline: 4/39; impact: 11/20) • 12.3% decrease of oral steroid prescription in the impact study (baseline: 20/39; impact 9/20) • Average cost per patient 2.4 times more in the impact study (baseline: 90.2 Coms; impact: 310.6 Coms)
Corticosteroid prescription, Tunisia Corticosteroid Baseline Impact Variation p-value drug study study in % No = 2341 No = 1422 ---------------------------------------------------------------------------------------- Any cortico-steroid 8.1% 5.2% - 35.8 < 0.001 * Bronchial inhalation 1.5% 1.3% - 20.0 0.617 *Nasal inhalation 0.2% 0.3% + 50.0 0.737 * Tablets 0.7% 0.4% - 43.0 0.246 *Injection 6.1% 3.6% - 41.0 < 0.002 ---------------------------------------------------------------------------------------- Among patients who were prescribed corticosteroid Inhaled Corticosteroid 18.9% 25.7% + 36.0 0.227 Average cost per patient2.7 DT2.9 DT+ 8.4% 0.505
Expected outcomes of PAL in countries • Contribution to improving national health policy since it defines health policy and intervention for the 1st leading cause of care demand in PHC setting (provision of an integrated package to 20 - 35% of patients) • Further step in DOTS quality improvement • Contribution to improving TB case detection, and quality of TB diagnosis • Maintaining the high profile of TB among respiratory conditions in daily practice • Strengthening the integration of TB control in PHC services • Improvement of the referral system for respiratory conditions and TB • Strengthening PHC services ( PHC attendance for respiratory conditions) • Reduction of drug prescription, particularly antibiotics and adjuvant drugs • Contribution to improving the competency of PHC workers • Contribution to improving health planning and formulation of resources needed within health system