Download
1 / 96
990 likes | 1.72k Views
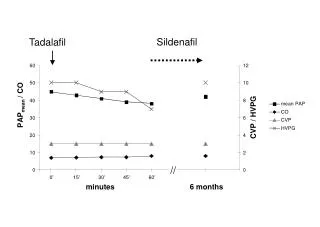
PAP . Positive airway pressure (PAP) adjuncts are used to mobilize secretions and treat atelectasis and include continuous positive airway pressure (CPAP) positive expiratory pressure (PEP) expiratory positive airway pressure (EPAP).

E N D
PAP • Positive airway pressure (PAP) adjuncts are used to mobilize secretions and treat atelectasis and include • continuous positive airway pressure (CPAP) • positive expiratory pressure (PEP) • expiratory positive airway pressure (EPAP). • Cough or other airway clearance techniques are essential components of PAP therapy when the therapy is intended to mobilize secretions
PAP: CPAP • The patient breathes from a pressurized circuit against a threshold resistor (water-column, weighted, or spring loaded) that maintains consistent preset airway pressures from 5 to 20 cm H2O during both inspiration and expiration • (By strict definition, CPAP is any level of above-atmospheric pressure.) • CPAP requires a gas flow to the airway during inspiration that is sufficient to maintain the desired positive airway pressure.
PAP: CPAP • Types of threshold resistors: all of these valves operate on the principle that the level of PAP generated within the circuit depends on the amount of resistance that must be overcome to allow gas to exit the exhalation valve. • They provide predictable, quantifiable, and constant force during expiration that is independent of the flow achieved by the patient during exhalation
PAP: CPAP • Underwater seal resistor: • expiratory port of the circuit is submerged under a column of water, the level of CPAP is determined by the height of the column • Weighted-ball resistor: • consists of a steel ball placed over a calibrated orifice, which is attached directly above the expiratory port of the circuit
PAP: CPAP • Spring-loaded: • rely on a spring to hold a disc or diaphragm down over the expiratory port of the circuit. • Magnetic valve resistors • contain a bar magnet that attracts a ferromagnetic disc seated on the expiratory port of the circuit the amount of pressure required to separate the disc from the magnets is determined be the distance between them.
PAP: PEP • The patient exhales against a fixed-orifice resistor, generating pressures during expiration that usually range from 10 to 20 cm H2O • PEP does not require a pressurized external gas source. • The amount of PEP varies with the size of the orifice and the level of expiratory flow produced by the patient. The smaller the orifice the greater the pressure.
PAP: PEP • Thus the patient must be encourage to generated a flow high enough to maintain expiratory pressure at 10-20 mm H2O • Ideal I:E of 1:3 or 1:4 • The patient should perform 10-20 breaths through the device and then perform 2-3 huff breath coughs • This should be repeated 5-10 times during a 15-20 minute session
PAP: EPAP • The patient exhales against a threshold resistor, generating preset pressures of 10 to 20 cm H2O (similar to CPAP expiration) • EPAP does not require a pressurized external gas source. • EPAP utilizing threshold resistors does not produce the same mechanical or physiologic effects that PEP does when a fixed orifice resistor is used. • Further study is necessary to determine how these differences affect clinical outcome.
IPPB, IPV, PEEP/CPAP and BIPAP October 1 & 8
IPPB • Intermittent Positive Pressure Breathing (IPPB) is a short-term breathing treatment where increased breathing pressures are delivered via ventilator to help treat atelectasis, clear secretions or deliver aerosolized medications • IPPB can include pressure- and time-limited, as well as pressure, time, and flow-cycled ventilation. • IPPB may be delivered to artificial airways and non-intubated patients.
IPPB • INDICATIONS:The need to improve lung expansionThe presence of clinically significant pulmonary atelectasis when other forms of therapy have been unsuccessful (incentive spirometry, chest physiotherapy, deep breathing exercises, positive airway pressure) or the patient cannot cooperate
IPPB • Inability to clear secretions adequately because of pathology that severely limits the ability to ventilate or cough effectively and failure to respond to other modes of treatment • The need for short-term ventilatory support for patients who are hypoventilating as an alternative to tracheal intubation and continuous mechanical ventilation
IPPB • The need to deliver aerosol medication. • IPPB may be used to deliver aerosol medications to patients with fatigue as a result of ventilatory muscle weakness (eg, failure to wean from mechanical ventilation, neuromuscular disease, kyphoscoliosis, spinal injury) or chronic conditions in which intermittent ventilatory support is indicated (eg, ventilatory support for home care patients and the more recent use of nasal IPPV for respiratory insufficiency)
IPPB • Assessment of need: • Presence of significant atelectasis • Reduced pulmonary function, reduced VC, VT • Neuromuscular disorders • Prevention of atelectasis Assessment of Outcome: • Minimum VT of at least 1/3 of predicted IC • Increase in FEV1 • More effective cough, CXR improved, BS improved
IPPB • CONTRAINDICATIONS:There are several clinical situations in which IPPB should not be used. With the exception of untreated tension pneumothorax, most of these contraindications are relative: • Increased ICP >15 mmHg • Hemodynamically unstable • Recent Facial, oral or skull surgery • Tracheoesphogeal fistula
IPPB • Recent Espohageal surgery • Active hemoptysis • Nausea • Air swallowing • Active TB • Blebs • Singulation (hiccups)
IPPB • Hazards/complications • Increased RAW and WOB • Barotrauma/pneumothorax • Nosocomial infection • Hypocarbia • Hemoptysis • Hyperoxia when O2 used as gas source • Gastric distension • Impaction of secretions
IPPB • Impendance of venous return • Air trapping Limitations of Device • Effects are short lived, lasting an hour • Delivery of medication is ineffective due to low delivering flow through nebulizer • Patient dependent • IPPB equipment is labor intensive • Limited portability
IPPB • IPPB is pneumatically powered • Patient triggered and pressure cycled • You set: Pressure limit, flow, sensitivity
IPPB • Given through a mouth piece or mask • Varying types, BIRD Mark series, PB
IPPB Setup Flow rate adjustment. Sensitivity adjustment Pressure adjustment Air mix, either 100% if pushed in or 80% pulled out Pressure manometer. Negative should not be more than -2, if it is adjust your sensitivity
IPPB • How the machine works: • In IPPB, we set a driving pressure [PIP] on the machine, and when the patient triggers the machine by decreasing the pressure in the line, gas starts to move down the tube into the mouth and airways. • When the preset PIP is reached, the gas flow shuts down immediately. The inspiratory phase has cycled off.
IPPB: Pressure • Pressure set on the IPPB will determine the pressure limit • Pressure is directly related to volume, increasing the pressure limit will increase the volume in the lung • Measure VT with • Venti-comp bag
IPPB Pressure • Pressure is typically started low, around 10-15 cmH2O and increased to achieve desired VT. Remember, IPPB is hyperinflation therapy, the goal is to exceed normal tidal volume ranges. • Once the machine is triggered on by the patient and pressure is reached (seen on manometer) the machine cycles off • Too much pressure can cause barotrauma
IPPB Flow • The flow setting on the IPPB dictates how fast the pressure limit is reached • High flow = low inspiratory time • Low flow = high inspiratory time • Start low around 5-10 L and increase depending on the desired inspiratory time • Normal times should be around 1-1.5 seconds for inspiration
IPPB Flow • To decrease the inspiratory time we need to increase the flow rate • To increase the inspiratory time, we need to decrease the flow rate • If we increase the PIP to increase the VT, sometimes the inspiratory time is too long and we have to increase the flow rate. • Remember that really fast flow rates will only cause increased RAW, so keep the inspiratory time between 1-1.5 seconds for adults. • Remember that the air mix mode involves air entrainment so the flow rate will be changed by changing the Fi02
IPPB Sensitivity • The sensitivity on the IPPB machine is manipulated by the dial on the left hand side of the machine. Increasing the “Inspiratory Effort” dial will make the machine less sensitive to the patients inspiratory trigger. This increases the magnetic pull inside the sub atmospheric side of the ,IPPB bird machine making it more difficult for the patient to trigger the machine on, increasing WOB
IPPB Sensitivity • Decreasing the “patient effort” dial will make the machine more sensitive to the patients inspiration. • This may cause “auto-triggering” if it is set too low. • Decreasing this dial creates less magnetic pull on the diaphragm in the middle of the machine
IPPB FIO2 • If you do not wish to deliver high FIO2 to the patient during the IPPB procedure, attach the machine to a air outlet, otherwise the only two FIO2 available are 100% or 80% with air dilution • NOTE: on the IPPB machine there is a APNEA- expiratory time setting, do not turn this on unless you want a back up rate.
Breathing while on IPPB • Remember, this is not ventilation. IPPB is a sustained maximal inspiration just like IS, so we do not need to breathe much faster than 6-8 bpm. The patient may breathe faster, but he can do so off the IPPB. • Rapid RR on the IPPB will increase chances of impeding venous return to the heart, reducing the amount of blood in the heart which would cause the patient to become tachycardiac in order the keep the same cardiac output.
Breathing while on IPPB • If the patient becomes light headed, dizzy or feels tingling in their fingers during the procedure- STOP and allow patient to rest, this is caused by the quick elimination of CO2 • Rapid RR will encourage air trapping, particularly in persons with increased RAW and wheezing—we need plenty of time to exhalation
Breathing while on IPPB • We need to allow for a 3-5 second inspiratory hold. • Remember this is a SMI, that includes a slow deep breath and inspiratory hold to get the gas and the medications deep into the periphery of the lung. The patient can take his mouth off the IPPB mouthpiece to do this breath hold—unless we need to measure the VT.
IPPB Troubleshooting • If you checked your PIP by watching the monometer while you occlude the patient connector, you will find most problems before attaching the machine to the patient. The pressure should go right to the PIP and stop immediately. The machine should not start just because you jiggle the tube. • Is the machine set for appropriate Fi02? • Is the sensitivity set for -2? • Check the PIP by monometer—not just the number on the dial • Is the circuit on nice and tight-do a tactile exam, not just looking at it. • If the SVN is set separately, is it set correctly?
IPPB Troubleshooting • Breath will not come on • 1. attach the high pressure line to the gas • 2. turn on the flow rate • 3. check the sensitivity; set the machine to trigger by itself [auto-cycling] then turn back a bit. • 4. does the patient have a tight seal? Mouth closed? Lips tight, nose closed or nose clips?
IPPB Troubleshooting • Breath starts too easily • 1. sensitivity is set too low. Auto-cycling is when the machine triggers itself just by jiggling the tube. • Breath will not end • 1. check the flow rate; too slow • 2. does the patient have a tight seal? Mouth closed? Lips tight, nose closed or nose clips? LEAKS • 3. check the mushroom valve, the nebulizer line, the nebulizer cup and the mainline for leaks.
IPPB Troubleshooting • Inhalation goes on past 1-1.5 seconds • 1. flow rate is too slow for this patient • 2. check for small leaks that prevent the pressure from rising. Look at the pressure on the monometer, there should be a steady rise in pressure • 3. if the pressure is wavering just lower than the PIP, the patient is ‘leading the machine.’ Ask him to relax & let the machine do the work. • He is inhaling too fast—also increase the flow rate per his comfort level • 4. if you moved from air mix to 100% Fi02, you lost the entrainment so the flow rate needs to be increased again
IPV • Intrapulmonary percussive ventilation (IPV) is a therapeutic modality designed to clear and maintain pulmonary airways. IPV is used to mobilize and clear retained secretions, assist in the resolution of atelectasis, and to deliver aerosolized medications. Oscillatory pulsations are delivery by the "Percussionator" which generates high frequency bursts of gas at rates of 100 to 300 cycles per minute (2 – 5 Hz). The mini bursts of air are delivered to the patient's airways at pressures of 10 – 20 cm H20, however this range may be adjusted to match the compliance and resistance of the lung and chest wall.
IPV • IPV was depicted as delivering “high flow mini-bursts of air along with bronchodilator to the lungs at a rate of 300–400 times per minute.” • operates at 1.7 Hz to 5 Hz and generates esophageal pressure and airflow oscillations • Treatments last about 15–20 min • This device is designed to be used in conjunction with conventional mechanical ventilation, if desired, or as a stand-alone treatment device. It can be used with a mouthpiece or mask, and it can also deliver aerosolized medication.
IPV • http://www.youtube.com/watch?v=ARJLALFf2e0 • Pneumatically powered • Nebulizer cup, uses a phasitron to create oscillations, bacterial filter, circuit- colored coded- connect lines to device • Set Drive pressure (based on patients compliance) • Set percussion level
PEEP • Positive end-expiratory pressure (PEEP) is the pressure in the lungs (alveolar pressure) above atmospheric pressure that exists at the end of expiration.The two types of PEEP are extrinsic PEEP (PEEP applied by a ventilator) and intrinsic PEEP (PEEP caused by a non-complete exhalation).
PEEP • There are three purposes to using PEEP: • 1) To prevent derecruitment, by returning the functional residual volume to the physiologic range. 2) To protect the lungs against injury during phasic opening an closing of atelectatic units. • 3) To assist cardiac performance, during heart failure, by increasing mean intrathoracic pressure.
PEEP • Applied (Extrinsic) PEEP — Applied PEEP can be given through invasive or non-invasive ventilation. • Works by increasing alveolar pressure to increase FRC, Mean Airway pressure and ultimatley improve compliance and improve oxygenation • PEEP is given in the range of about 3-5 and used to mitigate end-expiratory alveolar collapse. A higher level of applied PEEP (>5 cmH2O) is sometimes used to improve hypoxemia or reduce ventilator-associated lung injury in patients with acute lung injury, acute respiratory distress syndrome, or other types of hypoxemic respiratory failure
A: Collapsed alveoli on exhalation without PEEP B: Inflated alveoli on exhalation with PEEP C: Inflated alveoli on inspiration with PEEP
Auto-Peep (Intrinsic Peep) • Auto-PEEP is gas trapped in alveoli at end expiration, due to inadequate time for expiration, bronchoconstriction or mucus plugging. It increases the work of breathing. • Auto-PEEP is caused by gas trapped in alveoli at end expiration. This gas is not in equilibrium with the atmosphere and it exerts a positive pressure, increasing the work of breathing,
Auto-Peep (Intrinsic Peep) • The problem with gas trapping or “auto PEEP” is that gas trapped in the airways exerts a positive pressure, and normal gas transit cannot be reestablished until there is a pressure gradient from the mouth to the alveoli. Thus the patient must generate a much higher negative inspiratory pressure to open up dynamically compressed airways (to make the pressure within negative with respect to atmospheric pressure). • If auto-PEEP occurs during mechanical ventilation, the amount of time given over to expiration needs to be lengthened: either by reducing the respiratory rate or the inspiratory time, or both.