Download
1 / 18
180 likes | 390 Views

E N D
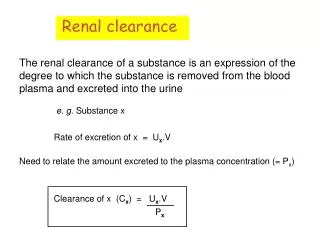
1. Prediction of metabolic clearance: CYP2C9 genotyping in epileptic patients on phenytoin
2. Epilepsy prevalence: 1 / 150 (2nd only to migraine)
excessive neuron stimulation within CNS
brain messages become halted / confused
seizure: burst of electrical activity in brain
generalised or partial Group of disorders characterized
Focal: simple or complex
Genralised: Convulsive (tonic-clonic)/Grand Mal
Nonconvulsive (absence)/Petite MalGroup of disorders characterized
Focal: simple or complex
Genralised: Convulsive (tonic-clonic)/Grand Mal
Nonconvulsive (absence)/Petite Mal
4. The Neuron axon - the long extension of a neuron that carries nerve impulses away from the body of the cell.
axon terminals - the hair-like ends of the axon
cell body - the cell body of the neuron; it contains the nucleus (also called the soma)
dendrites - the branching structure of a neuron that receives messages (attached to the cell body)
myelin sheath - the fatty substance that surrounds and protects some nerve fibers
node of Ranvier - one of the many gaps in the myelin sheath - this is where the action potential occurs during saltatory conduction along the axon
nucleus - the organelle in the cell body of the neuron that contains the genetic material of the cell
Schwann's cells - cells that produce myelin - they are located within the myelin sheath.
Green � axon
Red - dendriteaxon - the long extension of a neuron that carries nerve impulses away from the body of the cell.
axon terminals - the hair-like ends of the axon
cell body - the cell body of the neuron; it contains the nucleus (also called the soma)
dendrites - the branching structure of a neuron that receives messages (attached to the cell body)
myelin sheath - the fatty substance that surrounds and protects some nerve fibers
node of Ranvier - one of the many gaps in the myelin sheath - this is where the action potential occurs during saltatory conduction along the axon
nucleus - the organelle in the cell body of the neuron that contains the genetic material of the cell
Schwann's cells - cells that produce myelin - they are located within the myelin sheath.
Green � axon
Red - dendrite
5. Anti-epileptic drugs at the synapse
6. PHT clearance kinetics A 10% increase in dose may result in a 2-3 x C increase
A 10% increase in dose may result in a 2-3 x C increase
7. Dose / [PHT] relationship
8. Factors affecting phenytoin levels liver disease
GI disease
renal function
age Changes in hepatic blood flow do not alter phenytoin clearance because it is a low-extraction drug.10 However, loss of functional hepatocytes decreases phenytoin metabolism. Phenytoin accumulates as hepatic dysfunction increases.11 Because of decreased albumin production, liver disease is associated with decreased protein binding capacity for phenytoin. Further, bilirubin may compete for binding sites of the albumin molecule, further increasing the unbound concentration.12-17
The absorption of phenytoin is pH dependent and is maximal in the duodenum.9 Diseases that alter gut pH and decrease duodenal dwell time are likely to alter the absorption of phenytoin.
Phenytoin binding to plasma protein is decreased in patients with renal failure and hypoalbuminemia
Age-drugs common together too
Drugs: Chloramphenicol increases serum concentrations by 20%
Barbiturates acutely decrease phenytoin clearance (competitive), long-term enzyme induction increases clearance
Changes in hepatic blood flow do not alter phenytoin clearance because it is a low-extraction drug.10 However, loss of functional hepatocytes decreases phenytoin metabolism. Phenytoin accumulates as hepatic dysfunction increases.11 Because of decreased albumin production, liver disease is associated with decreased protein binding capacity for phenytoin. Further, bilirubin may compete for binding sites of the albumin molecule, further increasing the unbound concentration.12-17
The absorption of phenytoin is pH dependent and is maximal in the duodenum.9 Diseases that alter gut pH and decrease duodenal dwell time are likely to alter the absorption of phenytoin.
Phenytoin binding to plasma protein is decreased in patients with renal failure and hypoalbuminemia
Age-drugs common together too
Drugs: Chloramphenicol increases serum concentrations by 20%
Barbiturates acutely decrease phenytoin clearance (competitive), long-term enzyme induction increases clearance
10. CYP2C9
clinical relevance
metabolises 20 % of all drugs
warfarin, phenytoin, tolbutamide, ibuprofen
polymorphism
point mutations
*1 (wild type), *2 & *3 (poor metabolisers) Anti-coagulant, anti-convulsant, diabetes control, anti-inflammatoryAnti-coagulant, anti-convulsant, diabetes control, anti-inflammatory
11. Hypothesis � ability to clear Phenytoin is a
function of CYP2C9 genotype �
12. PCR-RFLP
13. Dose-Response
14. Determination of Km and Vmax
15. Pharmacokinetics
16. Summary
17. Conclusions CYP2C9 �poor metabolisers� can be phenotypically categorised:
lower Vmax
higher Km
maintained on lower PHT doses
PHT dose prediction should consider:
CYP2C9 genotype (CYP2C19)
Current medication
18. Acknowledgements Walton Centre for Neurology & Neurosurgery (WCNN)
Neurobiochemistry lab
Secretarial staff
Dr. David Britt (research governance)
Dr. Tony Marson, Dr. Siva Sathasivum, Prof. David Chadwick (epilepsy clinic)
University of Liverpool
Dr. Ana Alfirivic, Prof. Munir Pirmohamed (Pharmacology)
Jenny Austin, Dr. Lazlo Pazmany (Rheumatology, Clinical Sciences UHA)
University Hospital Aintree
Dr. Ian Watson