Download
1 / 38
410 likes | 450 Views
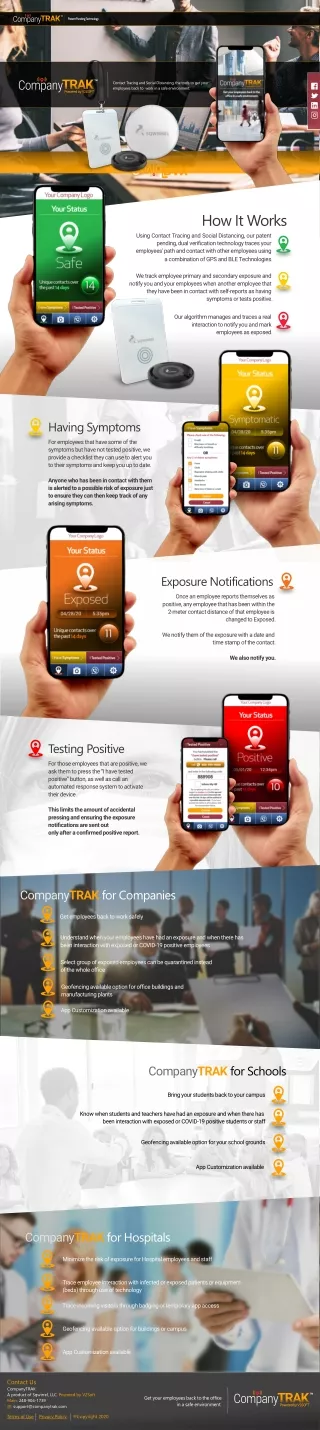
Learn about the steps involved in partner notification and contact tracing for disease control, focusing on HIV/AIDS investigation and sexually transmitted infections (STIs). Understand the purpose, use, and challenges of partner notification, as well as key strategies for effective case management. Explore how pre-interview analysis, initial interviews, and re-interviews help prevent disease transmission and provide necessary support. Discover the importance of cluster interviewing in expediting intervention processes.

E N D
Goals • Discuss the steps involved in partner notification or contact tracing
Finding a Needle in a Haystack • You need to find someone who has been exposed to a disease • Only know that a random person somewhere has been exposed • Identify someone who can tell you who was exposed and when exposure occurred • Your best source of information is person who exposed someone else to disease
Partner Notification or Contact Tracing • Can be very sensitive • Often involves discussing intimate relationships and diseases • Sexually transmitted infections (STIs) • Including HIV/AIDS
Partner Notification • “The process of locating and notifying partners that they have been exposed to a disease” • Partner in HIV/AIDS investigation: anyone who engaged in sexual activity or shared needles with original patient • Also referred to as contact tracing • More appropriate for diseases spread through non-sexual contact (tuberculosis, other communicable diseases)
Purpose of Partner Notification • Primary purpose is to prevent further transmission of disease. • More important with HIV/AIDS • Other goals: • to educate and treat infected individuals • to educate, test, treat (if needed) individuals exposed to infectious disease
Use of Partner Notification • Partner notification is used most commonly for syphilis and HIV/AIDS • Also for other STIs such as gonorrhea and chlamydia • Contact tracing used routinely for tuberculosis and disease outbreaks: • Measles, bacterial meningitis, Hepatitis A, severe acute respiratory syndrome • Contact tracing systems also developed for diseases like smallpox
Partner Notification of Sexually Transmitted Infections • Guided by state law • Variations in the process depending on the state, health department, and type of disease • CDC recommends following steps for effective provider referral case management of STIs
Partner Notification of Sexually Transmitted Infections Pre-Interview Analysis • Reviews medical and case data to learn: • Status of the case (new or recurrent) • Medical information on the patient • Pregnancy status for women • Issues unique to patient - embarrassment, sexual orientation, drug use, cooperativeness, attitude, history of domestic violence, psychiatric issues • Establishes time patient could have spread disease • Begins with earliest date patient could have been infected • Ends with date of treatment • May be obtained from health department, physician, hospital, jail, prison records
Partner Notification of Sexually Transmitted Infections Initial Interview • Purpose is to prevent further transmission of disease through identification and communication with index patient and partner(s) • Educating patient about seriousness of disease and importance of cooperation • Providing patient with risk reduction plan and appropriate community referrals (e.g., substance abuse treatment centers, prenatal care) • Eliciting partner information from patient
Partner Notification of Sexually Transmitted Infections Initial Interview • Partner elicitation accomplished by asking patient for: • Names (and nicknames) of sexual and needle-sharing partners • Frequency and dates of exposure • Address and phone/beeper numbers • Place of employment • Physical description • Who partner lives with, where partner hangs out • Whether partner has been incarcerated
Partner Notification of Sexually Transmitted Infections Initial Interview • Partner elicitation • Can also provide information about other high-risk individuals ( “suspects”) who are not partners but may need medical evaluation • Goal to obtain information to find partners and suspects so interviewer can provide education and risk-reduction counseling, refer for testing and treatment
Interviewing Challenges • Often interviewing is not straightforward • Challenging situations include: • Finding a homeless individual who has no home address, only information about what soup kitchen or shelter he/she frequents • Finding a prostitute based only on “street name,” physical description, and where usually works • Working in dangerous neighborhoods or places (e.g., crack houses)
Partner Notification of Sexually Transmitted Infections Re-Interview • Re-interview often needed to: • Gather more partner information • Re-emphasize risk reduction and referrals • Clarify illogical statements • Elicit additional partners or suspects • Usually done within several days of initial interview
Partner Notification of Sexually Transmitted Infections Case Closure • Case is closed when investigator and supervisor agree that all reasonable steps to intervene in disease transmission have been taken
Cluster Interviewing • Cluster interviewing expedites intervention process when there is not enough partner information to allow investigators to reach partners individually • Gather information about previously unnamed partners or cases and any persons who might benefit from a medical examination • May identify partners whom the case patient is unwilling to identify
Cluster Interviewing • Cluster interview attempts to find others at risk by interviewing patient's partners and suspects not known to be infected • Does not disclose names of individuals infected or at risk of infection, conveys only that syphilis has been diagnosed in the area • Provides each person with information about syphilis and encourages person to get tested • Emphasizes that person can decrease risk by offering names of partners and other high-risk individuals to be interviewed • Information may be used to determine risk profiles and geographic locations of target groups for screening
Cluster Interviews - Example Tuberculosis in a Transgender Network • Summer 1998: Baltimore City Health Department notified of 4 cases of TB among young men • All part of a transgender social network, participated in “houses” (social guilds for men who have sex with men and transgender persons) • Began with traditional contact investigation • Identified 14 contacts • Developed profile of people participating in social network: history of membership in a “house,” attendance at specific events, reported cross-dressing • Process similar to cluster interviewing: people identified were not necessarily close contacts of confirmed TB cases • Identified 91 contacts • Found 6 additional cases of TB
Partner Notification/Contact Tracing of Tuberculosis • Contact tracing for non-sexually transmitted diseases similar to that for STIs • CDC and the National Tuberculosis Controllers Association published guidelines for TB contact tracing in 2005 • Recommend that contact investigation be conducted when patient has confirmed or suspected pulmonary, laryngeal, or pleural TB, and sputum smear or chest radiograph indicates TB
Partner Notification/Contact Tracing of Tuberculosis • First step is to gather background information about patient from medical record, reporting physician, or hospital infection control nurse • Background information used to determine infectious period for patient
Partner Notification/Contact Tracing of Tuberculosis Interview • Should occur within 1 business day of reporting for infectious patient, within 3 business days of reporting for non-infectious patient • Should be conducted in person • Gathers information about places where disease transmission could have occurred: patient’s home and congregate settings (schools, nursing homes, correctional facilities, homeless shelters) • Asks for names, phone numbers, addresses of people who may have been exposed • Interviewer may prioritize the places of likely transmission, follow up with another interview
Partner Notification/Contact Tracing of Tuberculosis Site Visit • Visit places of likely disease transmission to: • Identify additional contacts, including children • Determine the likelihood of disease transmission • Visit to homeless shelter to see how many people sleep in same room, how much ventilation, whether people eat together in a common area, whether shelter provides screening or other health services)
Partner Notification/Contact Tracing of Tuberculosis Prioritizing Contacts • Most important criteria: • Age under 5 years • Compromised immune status, such as HIV infection • Secondary criteria: • Type of exposure • Other medical conditions such as diabetes • Exposure classified by amount of air volume shared • Smallest amount (inside a car) indicates high level of exposure • Largest size (larger than a house) indicates lower likelihood of exposure
Contact Tracing of Tuberculosis - Example TB Investigation in Ohio • January 2005: woman came to Ashtabula County Health Department to have tuberculin skin test • Test was positive; subsequently developed active tuberculosis, as indicated by chest radiograph and a positive sputum smear. • Public health nurses interviewed to obtain information about contacts; all contacts tested negative for TB • Additional cases of TB reported to health department in March 2005 • Son of one of the patients had been experiencing symptoms consistent with TB for previous 4 years; medical professionals had suspected TB but none started patient on TB treatment or notified health department • The complete contact investigation uncovered 6 cases of TB after skin testing of 81 exposed contacts
Partner Notification in an Outbreak • Partner notification/contact tracing critical during outbreak • Can identify additional cases infected with disease and pinpoint possible sites of disease transmission
Partner Notification in an Outbreak San Francisco Syphilis Outbreak • Summer 1999: San Francisco Department of Public Health learned of 2 cases of early-stage syphilis • Both patients met most of sexual partners in same Internet chat room • Patients did not have any information about many partners other than Internet screen names • Sent e-mails to screen names and requested reply • Partners who responded advised to undergo medical evaluation • Identified 5 additional cases of syphilis
Responsibility for Partner Notification • Depending on situation and persons involved, either a public health professional or the patient may notify partner(s). • Generally 3 ways to approach partner notification: • Health care provider • Patient • Contract referral
Responsibility for Partner Notification Provider Referral • Public health professional or health care provider notifies partners of potential disease exposure • Notification is confidential, with consent of infected person • Notification for sexually transmitted diseases, • Often done by disease intervention specialist (public health professional specially trained in partner notification) • Clinicians or other public health department staff • Notification for TB contacts: • Some health departments have team members devoted to contact tracing • Public health nurses, other members of multidisciplinary investigation teams • When diagnosed in hospital, infection control practitioner or employee health nurse
Responsibility for Partner Notification Self/Patient Referral • Patient takes responsibility for notifying partners of potential exposure, referring them to medical care • Public health department staff work with patients to help them prepare for interactions with partners Contract Referral • Patient agrees to notify and refer to medical care all partners within a certain time period • If patient fails to do so, provider has permission to notify and refer partners
Training of Investigators • Training varies depending on background and job description of investigator • Some receive intensive training through state health department or CDC • CDC has contact tracing self-study module • If responsibilities include drawing blood, should be trained in Occupational Safety and Health Administration (OSHA) standards and venipuncture • Role playing with practice interviews • HIV counseling and testing • Cconfidentiality • Hands-on field experience with a mentor
Training of Investigators • Investigator must know how to: • Take sexual histories • Effectively elicit partners’ names • Identify and locate contacts • Refer persons for testing, treatment, and social services • Educate and counsel persons on high risk behavior • Must be able to apply skills with individuals who often do not trust them, may not be particularly happy to see them, are concerned about their confidentiality, and may not be motivated to cooperate • Must gain the trust of patient and maintain confidentiality • Must be familiar with epidemiology of the disease
Legal Authority for Partner Notification • Legal authority for partner notification of sexually transmitted infections resides with states • Legal authority for mandatory disease reporting is derived from state law; states may have different organizational structures and approaches depending on state laws • All 50 states require that certain diseases be reported to state or local health department • List of reportable diseases varies by state
Confidentiality • Maintaining patient confidentiality is imperative • Promotes trusting relationship between investigator and patient • Required by law to protect the privacy of the patient • Always interview cases and partners in private • Try to notify partners face to face • Never reveal identity of original case to partner • Do not leave verbal or written messages that mention disease • Do not give confidential information to others • Investigation documentation is confidential material • In addition to state and federal laws, each public health department has specific guidelines and legal regulations
Summary • Contact tracing may be carried out for different infectious diseases (e.g., HIV, syphilis, TB) • May be done by provider, patient, or contract referral • While specific procedures differ by state, primary goal is to intervene in transmission of infectious disease • Education, testing, treatment are additional goals of contact tracing
References • Centers for Disease Control and Prevention. Program operations guidelines for STD prevention: Partner services. Available at: http://www.cdc.gov/std/program/partners.pdf. Accessed September 26, 2007. • Hogben M. Partner notification for sexually transmitted diseases. Clinl Infect Dis. 2007;44(suppl 3):S160-S174. • Golden MR, Hogben M, Handsfield HH, St. Lawrence JS, Potterat JJ, Holmes KK. Partner notification for HIV and STD in the United States: Low coverage for gonorrhea, chlamydial infection, and HIV. Sex Trans Dis. 2003;30:490-496. • Centers for Disease Control and Prevention. Smallpox response plan and guidelines (version 3.0). Available at: http://www.bt.cdc.gov/agent/smallpox/response-plan/index.asp. Accessed October 25, 2007.
References • Centers for Disease Control and Prevention. Cluster of HIV-infected adolescents and young adults – Mississippi, 1999. MMWR Morb Mortal Wkly Rep. 2000;49:861-864. • Centers for Disease Control and Prevention. Guidelines for the investigation of contacts of persons with infectious tuberculosis. MMWR Recomm Rep. 2005;54:1-43. • Kettunen CM, Sunmonu Y, Hodgkinson AL, et al. Contact investigation of a case of active tuberculosis in the community. Am J Infect Control. 2007;35:421-424. • Klausner JD, Wolf W, Fischer-Ponce L, Zolt I, Katz MH. Tracing a syphilis outbreak through cyberspace. JAMA. 2000;284:447-449.
References • Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections among competitive sports participants – Colorado, Indiana, Pennsylvania, and Los Angeles County, 2002-2003. MMWR Morb Mort Wkly Rep. 2003;52:793-795.Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/ mm5233a4.htm. Accessed December 15, 2006. • Centers for Disease Control and Prevention. Use of quarantine to prevent severe acute respiratory syndrome – Taiwan, 2003. MMWR Morb Mort Wkly Rep. 2003;52:680-683. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5229a2.htm. Accessed December 15, 2006. • Centers for Disease Control and Prevention. Efficiency of quarantine during an epidemic of severe acute respiratory syndrome – Beijing, China, 2003. MMWR Morb Mort Wkly Rep. 2003;52:1037-1040. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/ mm5243a2.htm. Accessed December 15, 2006.
References • Macke BA, Maher JE. Partner notification in the United States: An evidence-based review. Am J Prev Med. 1999; 17:230-242. • Wilce M, Shrestha-Kuwahara R, Taylor Z, Qualls N, Marks S. Tuberculosis contact investigation policies,practices and challenges in 11 U.S. Communities. J Public Health Manag Pract. 2002;8:69-78. • Centers for Disease Control and Prevention. Self-study modules on tuberculosis. Module 6: Contact investigations for tuberculosis. Available at: http://www.cdc.gov/tb/pubs/ssmodules/module6/ss6contents.htm. Accessed September 26, 2007. • Teutsch SM, Churchill RE, eds. Principles and Practice of Public Health Surveillance. New York, NY: Oxford University Press; 2000.