Download
1 / 22
240 likes | 431 Views
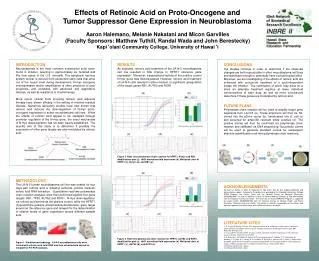
Cooperative Clinical Trials with 13-Cis-Retinoic Acid in Neuroblastoma. Katherine K. Matthay, M.D University of California, San Francisco Children’s Oncology Group. 13-cis-RA Clinical Studies in Neuroblastoma.

E N D
Cooperative Clinical Trials with 13-Cis-Retinoic Acid in Neuroblastoma Katherine K. Matthay, M.D University of California, San Francisco Children’s Oncology Group
13-cis-RAClinical Studies in Neuroblastoma • CCG Phase II trial in recurrent high-risk neuroblastoma employing adult daily continuous dosing (100 mg/m2) • Multi-institution Phase I to dose-escalate intermittent (2 weeks/mo) 13-cis-RA in patients after ABMT • CCG-3891 Phase III randomized trial, high-risk neuroblastoma in first response
13-cis-RA Dose Escalation • 100 mg/m2 for 14/28 days divided b.i.d. • 125 mg/m2 for 14/28 days divided b.i.d. • 160 mg/m2 for 14/28 days divided b.i.d. • 200 mg/m2 for 14/28 days divided b.i.d.
Dose Limiting Toxicity • 160 mg/m2: n=24 patients/144 courses • Skin grade 3: n=3 • Hepatic grade 3: n=1 • Neutropenia grade 3: n=1 • Hypercalcemia grade 4: n=1 • 200 mgm2: DLT in 6/9 patients/ 48 courses • Skin grade 3: n=2 • Hypercalcemia: n=3 (2 were grade 4) • Anemia/thrombocytopenia grade 3: n=1
Common Grade 1 and 2 Toxicities • Cheilitis • Skin • Diarrhea • Hypertriglyceridemia • Elevated Transaminase • Hypercalcemia
Pharmacokinetics vs Toxicity • Peak Plasma Level ≥ 10 µM • 6/8 grade 3-4 toxicity (75%) • Peak Plasma Level <10 µM • 3/20 grade 3-4 toxicity (15%)
13-cis-RA Phase I Clinical Responses • 10 patients with assessable disease • 4 achieved CR (3 in bone marrow) • 5 developed PD • 1 had SD
Summary of Pharmacokinetics • A linear increase with increasing daily dosage in • Plasma peak and trough • AUC • The mean peak plasma level at the MTD of 160 mg/m2 was greater than 5 µM • Peak plasma levels ≥ 10 µM were associated with grade 3-4 clinical toxicities
Phase I Study of 13-cis-RAConclusions • The MTD of intermittent 13-CRA is 160 mg/m2, divided twice daily • Dose limiting toxicities were hypercalcemia, gastrointestinal, hematopoietic and skin • Plasma concentrations of 5 uM, which produce sustained growth arrest of neuroblastoma in vitro, can be achieved with acceptable clinical toxicity
13-cis-Retinoic Acid After Intensive Consolidation Therapy for Neuroblastoma Improves Event-Free SurvivalA Randomized Children’s Cancer Group Study K Matthay, Chair Results of the 2nd Randomization for CCG-3891 Testing effect of 13-cis-RA Therapy on Event-Free Survival
CCG-3891 Specific Aims • Compare by prospective randomization, the efficacy and toxicity of consolidation chemotherapy vs intensive chemoradiotherapy with ABMT • Determine by prospective randomization the effects of 13-cis-retinoic acid on minimal residual disease and relapse-free survival
CCG-3891 Induction Chemotherapy 13-cis-RA Consolidation Chemotherapy Marrow harvest and purging Surgery Local Radiation No 13-cis-RA Dx Myeloablative Chemo/TBI ABMT 13-cis-RA No 13-cis-RA Randomize 8 Weeks Randomize 34 Weeks
CCG-3891 Patient Characteristics • 539 Patients • Study open from Jan 1991 to Apr 1996 • Average age at diagnosis = 2.5 years (range 3 months to 17 years) • 85 % Stage IV • 40 % with MYCN genomic amplification
Toxicities in 173 Patients Treated with 13-cis-RA 15% First 3 Months 9% Second 3 Months
CCG-3891 Overall Survival From Time of First Randomization
CCG-3891 Event-Free Survival From Time of 2nd Randomization
CCG-3891 Overall Survival From Time of 2nd Randomization
CCG-3891 Conclusions • Both myeloablative therapy and post-myeloablative therapy with high-dose, pulse 13-cis-retinoic acid improved event-free survival for high-risk neuroblastoma • There was an increase in overall survival for both ABMT and 13-cis-RA, which is highest for patients randomized to receive myeloablative therapy followed by 13-cis-RA