Download
1 / 1
10 likes | 160 Views
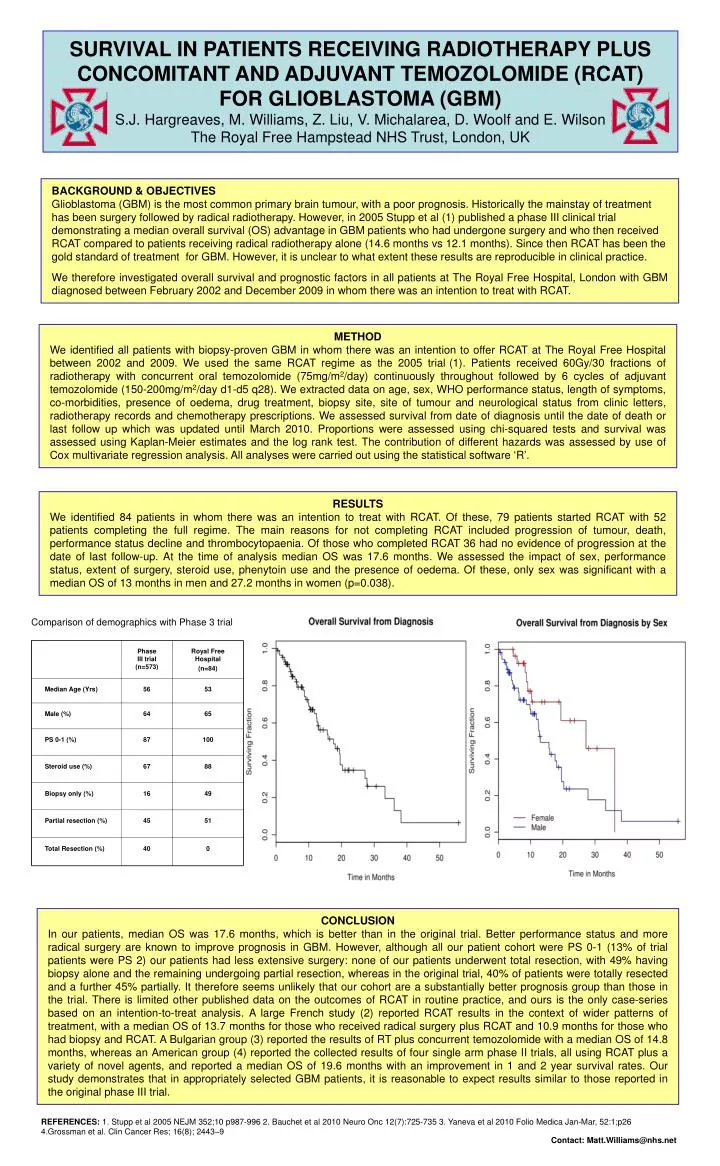
Phase III trial (n=573) . Royal Free Hospital (n=84) . Median Age (Yrs) . 56. 53. Male (%) . 64. 65. PS 0-1 (%) . 87. 100. Steroid use (%) . 67. 88. Biopsy only (%) . 16. 49. Partial resection (%) . 45. 51. Total Resection (%) . 40. 0.

E N D
Phase III trial (n=573) Royal Free Hospital (n=84) Median Age (Yrs) 56 53 Male (%) 64 65 PS 0-1 (%) 87 100 Steroid use (%) 67 88 Biopsy only (%) 16 49 Partial resection (%) 45 51 Total Resection (%) 40 0 SURVIVAL IN PATIENTS RECEIVING RADIOTHERAPY PLUS CONCOMITANT AND ADJUVANT TEMOZOLOMIDE (RCAT) FOR GLIOBLASTOMA (GBM)S.J. Hargreaves, M. Williams, Z. Liu, V. Michalarea, D. Woolf and E. WilsonThe Royal Free Hampstead NHS Trust, London, UK BACKGROUND & OBJECTIVESGlioblastoma (GBM) is the most common primary brain tumour, with a poor prognosis. Historically the mainstay of treatment has been surgery followed by radical radiotherapy. However, in 2005 Stupp et al (1) published a phase III clinical trial demonstrating a median overall survival (OS) advantage in GBM patients who had undergone surgery and who then received RCAT compared to patients receiving radical radiotherapy alone (14.6 months vs 12.1 months). Since then RCAT has been the gold standard of treatment for GBM. However, it is unclear to what extent these results are reproducible in clinical practice. We therefore investigated overall survival and prognostic factors in all patients at The Royal Free Hospital, London with GBM diagnosed between February 2002 and December 2009 in whom there was an intention to treat with RCAT. METHODWe identified all patients with biopsy-proven GBM in whom there was an intention to offer RCAT at The Royal Free Hospital between 2002 and 2009. We used the same RCAT regime as the 2005 trial(1). Patients received 60Gy/30 fractions of radiotherapy with concurrent oral temozolomide (75mg/m2/day) continuously throughout followed by 6 cycles of adjuvant temozolomide (150-200mg/m2/day d1-d5 q28). We extracted data on age, sex, WHO performance status, length of symptoms, co-morbidities, presence of oedema, drug treatment, biopsy site, site of tumour and neurological status from clinic letters, radiotherapy records and chemotherapy prescriptions. We assessed survival from date of diagnosis until the date of death or last follow up which was updated until March 2010. Proportions were assessed using chi-squared tests and survival was assessed using Kaplan-Meier estimates and the log rank test. The contribution of different hazards was assessed by use of Cox multivariate regression analysis. All analyses were carried out using the statistical software ‘R’. RESULTSWe identified 84 patients in whom there was an intention to treat with RCAT. Of these, 79 patients started RCAT with 52 patients completing the full regime. The main reasons for not completing RCAT included progression of tumour, death, performance status decline and thrombocytopaenia. Of those who completed RCAT 36 had no evidence of progression at the date of last follow-up. At the time of analysis median OS was 17.6 months. We assessed the impact of sex, performance status, extent of surgery, steroid use, phenytoin use and the presence of oedema. Of these, only sex was significant with a median OS of 13 months in men and 27.2 months in women (p=0.038). Comparison of demographics with Phase 3 trial CONCLUSIONIn our patients, median OS was 17.6 months, which is better than in the original trial. Better performance status and more radical surgery are known to improve prognosis in GBM. However, although all our patient cohort were PS 0-1 (13% of trial patients were PS 2) our patients had less extensive surgery: none of our patients underwent total resection, with 49% having biopsy alone and the remaining undergoing partial resection, whereas in the original trial, 40% of patients were totally resected and a further 45% partially. It therefore seems unlikely that our cohort are a substantially better prognosis group than those in the trial. There is limited other published data on the outcomes of RCAT in routine practice, and ours is the only case-series based on an intention-to-treat analysis. A large French study (2) reported RCAT results in the context of wider patterns of treatment, with a median OS of 13.7 months for those who received radical surgery plus RCAT and 10.9 months for those who had biopsy and RCAT. A Bulgarian group (3) reported the results of RT plus concurrent temozolomide with a median OS of 14.8 months, whereas an American group (4) reported the collected results of four single arm phase II trials, all using RCAT plus a variety of novel agents, and reported a median OS of 19.6 months with an improvement in 1 and 2 year survival rates. Our study demonstrates that in appropriately selected GBM patients, it is reasonable to expect results similar to those reported in the original phase III trial. REFERENCES: 1. Stupp et al 2005 NEJM 352;10 p987-996 2. Bauchet et al 2010 Neuro Onc 12(7):725-735 3. Yaneva et al 2010 Folio Medica Jan-Mar, 52:1;p26 4.Grossman et al. Clin Cancer Res; 16(8); 2443–9 Contact: Matt.Williams@nhs.net