Download
1 / 1
10 likes | 144 Views
Pathophysiology of Migraine-Related Dizziness Joseph Furman 1,3,4 , Dawn Marcus 2 , Patrick Sparto 3,1,4 , Mark Redfern 4,1,3 , and J. Richard Jennings 5

E N D
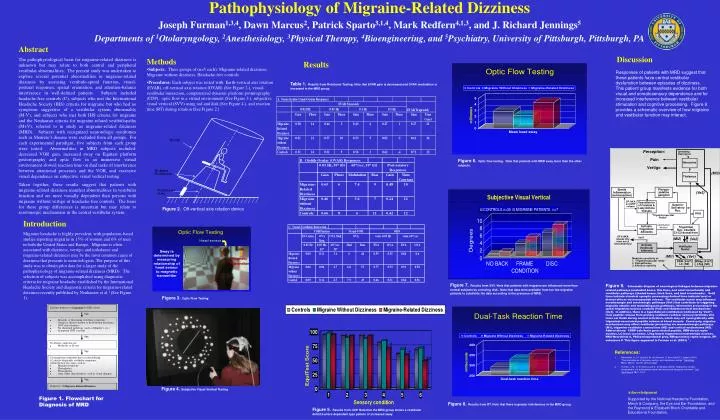
Pathophysiology of Migraine-Related Dizziness Joseph Furman1,3,4, Dawn Marcus2, Patrick Sparto3,1,4, Mark Redfern4,1,3, and J. Richard Jennings5 Departments of 1Otolaryngology, 2Anesthesiology, 3Physical Therapy, 4Bioengineering, and 5Psychiatry, University of Pittsburgh, Pittsburgh, PA Abstract The pathophysiological basis for migraine-related dizziness is unknown but may relate to both central and peripheral vestibular abnormalities. The present study was undertaken to explore several potential abnormalities in migraine-related dizziness by assessing vestibulo-spinal function, visual-postural responses, spatial orientation, and attention-balance interference in well-defined patients. Subjects included headache-free controls (C), subjects who met the International Headache Society (IHS) criteria for migraine but who had no symptoms suggestive of a vestibular system abnormality (M-V), and subjects who met both IHS criteria for migraine and the Neuhauser criteria for migraine-related vestibulopathy (M+V), referred to in study as migraine-related dizziness (MRD). Subjects with recognized neurotologic syndromes such as Meniere’s disease were excluded from all groups. For each experimental paradigm, five subjects from each group were tested. Abnormalities in MRD subjects included: decreased VOR gain, increased sway on Equitest platform posturography and optic flow in an immersive virtual environment slowed reaction time on dual tasks of interference between attentional processes and the VOR, and excessive visual dependence on subjective visual vertical testing. Taken together, these results suggest that patients with migraine-related dizziness manifest abnormalities in vestibular function and are more visually dependent than persons with migraine without vertigo or headache-free controls. The basis for these group differences is uncertain but may relate to serotonergic mechanisms in the central vestibular system. Discussion • Methods • Subjects: Three groups of (n=5 each): Migraine-related dizziness; • Migraine without dizziness; Headache-free controls • Procedures: Each subject was tested with: Earth-vertical axis rotation (EVAR), off-vertical axis rotation (OVAR) (See Figure 2.), visual-vestibular interaction, computerized dynamic platform posturography (CDP), optic flow in a virtual environment (See Figure 3.), subjective visual vertical (SVV) using rod and disk (See Figure 4.), and reaction time (RT) during rotation (See Figure 2.) Results Responses of patients with MRD suggest that these patients have central vestibular dysfunction between episodes of dizziness. This patient group manifests evidence for both visual and somatosensory dependence and for increased interference between vestibular stimulation and cognitive processing. Figure 9 provides a schematic overview of how migraine and vestibular function may interact. Table 1.Results from Rotational Testing. Note that EVAR gain is decreased and OVAR modulation is increased in the MRD group. Figure 6.Optic flow testing. Note that patients with MRD sway more than the other subjects. Figure 2.Off-vertical axis rotation device Introduction Migraine headache is highly prevalent, with population-based studies reporting migraine in 15% of women and 6% of men in both the United States and Europe. Migraine is often associated with dizziness, vertigo, and imbalance and migraine-related dizziness may be the most common cause of dizziness that presents to neurotologists. The purpose of this study was to obtain pilot data for a larger study of the pathophysiology of migraine-related dizziness (MRD). The selection of subjects was accomplished using diagnostic criteria for migraine headache established by the International Headache Society and diagnostic criteria for migraine-related dizziness recently published by Neuhauser et al 1 (See Figure 1). Figure 9.Schematic diagram of neurological linkages between migraine-related pathways (unshaded boxes, thin lines, and small arrowheads) and vestibular pathways (shaded boxes, thick lines, and bold arrowheads). Solid lines indicate classical synaptic processing; dashed lines indicate local or distant effects via neuropeptide release. The vestibular nuclei may influence noradrenergic and serotonergic pathways (Ve1) that contribute to triggering migraine attacks and modulating pain pathways, information processing in the spinal trigeminal nucleus caudalis (Ve2) and thalamocortical mechanisms (Ve3). In addition, there is a hypothetical contribution (indicated by 'Ve4?') from peptide release from primary vestibulo-cochlear sensory terminals into inner ear fluids during normal activation, which may act synergistically with trigeminal-associated peptide release at blood vessels. Conversely, migraine mechanisms may affect vestibular processing via monoaminergic pathways (M1), trigemino-vestibular connections (M2) and cortical mechanisms (M3). Abbreviations: CGRP-calcitonin gene-related peptide, DRN-dorsal raphe nucleus, LC-locus coeruleus, LTeg-lateral tegmental noradrenergic neurons, NKA-Neurokinin A, PAG-periaqueductal gray, RMag-nucleus raphe magnus, SP-substance P. This figure appeared in Furman et al. (2003) 2 . Figure 7.Results from SVV. Note that patients with migraine are influenced more than normal subjects by a moving disk. Note that data were available from too few migraine patients to subdivide the data according to the presence of MRD. Figure 3. Optic Flow Testing • References: • Neuhauser, H., M. Leopold, M. von Brevern, G. Arnold and T. Lempert (2001). "The interrelations of migraine, vertigo, and migrainous vertigo." Neurology56(4): 436-41. Current opinion paper • Furman, J. M., D. A. Marcus and C. D. Balaban (2003). "Migrainous vertigo: development of a pathogenetic model and structured diagnostic interview." Curr Opin Neurol16(1): 5-13. Figure 4. Subjective Visual Vertical Testing Acknowledgement Supported by the National Headache Foundation, Merck & Company, the Eye and Ear Foundation, and the Raymond & Elizabeth Bloch Charitable and Educational Foundation. Figure 1. Flowchart for Diagnosis of MRD Figure 8.Results from RT. Note that there is greater interference in the MRD group. Figure 5.Results from CDP. Note that the MRD group shows a vestibular deficit/surface dependent type pattern of increased sway.