Download
1 / 2
40 likes | 283 Views
CI to Triptans: Uncontrolled HTN CHD CVD PVD RF for the above. In Menstrually related migraine: Mefanamic acid 500mg tds-qds or Naproxen 500mg bd during menstruation. Or COCP or transdermal oestrogen as long as there is no aura.

E N D
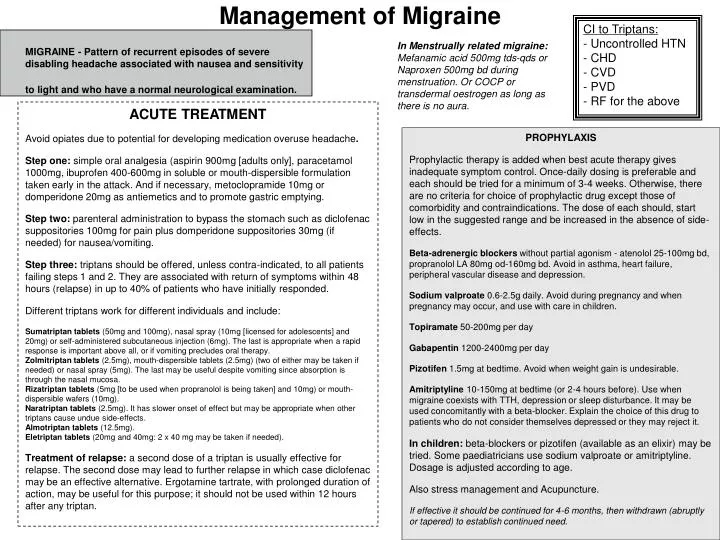
CI to Triptans: • Uncontrolled HTN • CHD • CVD • PVD • RF for the above In Menstrually related migraine: Mefanamic acid 500mg tds-qds or Naproxen 500mg bd during menstruation. Or COCP or transdermal oestrogen as long as there is no aura. MIGRAINE - Pattern of recurrent episodes of severe disabling headache associated with nausea and sensitivity to light and who have a normal neurological examination. Management of Migraine ACUTE TREATMENT Avoid opiates due to potential for developing medication overuse headache. Step one: simple oral analgesia (aspirin 900mg [adults only], paracetamol 1000mg, ibuprofen 400-600mg in soluble or mouth-dispersible formulation taken early in the attack. And if necessary, metoclopramide 10mg or domperidone 20mg as antiemetics and to promote gastric emptying. Step two: parenteral administration to bypass the stomach such as diclofenac suppositories 100mg for pain plus domperidone suppositories 30mg (if needed) for nausea/vomiting. Step three: triptans should be offered, unless contra-indicated, to all patients failing steps 1 and 2. They are associated with return of symptoms within 48 hours (relapse) in up to 40% of patients who have initially responded. Different triptans work for different individuals and include: Sumatriptan tablets (50mg and 100mg), nasal spray (10mg [licensed for adolescents] and 20mg) or self-administered subcutaneous injection (6mg). The last is appropriate when a rapid response is important above all, or if vomiting precludes oral therapy. Zolmitriptan tablets (2.5mg), mouth-dispersible tablets (2.5mg) (two of either may be taken if needed) or nasal spray (5mg). The last may be useful despite vomiting since absorption is through the nasal mucosa. Rizatriptan tablets (5mg [to be used when propranolol is being taken] and 10mg) or mouth-dispersible wafers (10mg). Naratriptan tablets (2.5mg). It has slower onset of effect but may be appropriate when other triptans cause undue side-effects. Almotriptan tablets (12.5mg). Eletriptan tablets (20mg and 40mg: 2 x 40 mg may be taken if needed). Treatment of relapse: asecond dose of a triptan is usually effective for relapse. The second dose may lead to further relapse in which case diclofenac may be an effective alternative. Ergotamine tartrate, with prolonged duration of action, may be useful for this purpose; it should not be used within 12 hours after any triptan. PROPHYLAXIS Prophylactic therapy is added when best acute therapy gives inadequate symptom control. Once-daily dosing is preferable and each should be tried for a minimum of 3-4 weeks. Otherwise, there are no criteria for choice of prophylactic drug except those of comorbidity and contraindications. The dose of each should, start low in the suggested range and be increased in the absence of side-effects. Beta-adrenergic blockers without partial agonism - atenolol 25-100mg bd, propranolol LA 80mg od-160mg bd. Avoid in asthma, heart failure, peripheral vascular disease and depression. Sodium valproate 0.6-2.5g daily. Avoid during pregnancy and when pregnancy may occur, and use with care in children. Topiramate 50-200mg per day Gabapentin 1200-2400mg per day Pizotifen 1.5mg at bedtime. Avoid when weight gain is undesirable. Amitriptyline 10-150mg at bedtime (or 2-4 hours before). Use when migraine coexists with TTH, depression or sleep disturbance. It may be used concomitantly with a beta-blocker. Explain the choice of this drug to patients who do not consider themselves depressed or they may reject it. In children: beta-blockers or pizotifen (available as an elixir) may be tried. Some paediatricians use sodium valproate or amitriptyline. Dosage is adjusted according to age. Also stress management and Acupuncture. If effective it should be continued for 4-6 months, then withdrawn (abruptly or tapered) to establish continued need.
RED FLAGS - Need specialist referral New onset or change in headache in patients over 50 Thunderclap headache Focal neurological symptoms Non-focal neurological disturbance eg, cognition Abnormal Neurological exam Headache which changes with posture Headache waking up form sleep Headache ppt by valsava maneouvre or exercise Patients with RF for venous sinus thrombosis Jaw claudication or visual disturbance Neck stiffness Fever Headache in patient with cancer Headache in patient with HIV infection • Tension-type headache • Bilateral headache that is non-disabling where there is a normal neurological examination. • Drug therapy has limited scope but is effective in some patients: • Symptomatic treatment with over-the-counter analgesics is appropriate for episodic TTH occurring on <2 days per week: aspirin 600-900mg, ibuprofen 400mg or paracetamol 1000mg • Codeine and dihydrocodeine should be avoided. • A 3-week course of naproxen 250-500mg bd may interrupt frequently recurring or unremitting headaches • PROPHYLAXIS • Amitriptyline is the prophylactic treatment of choice for frequent episodic or chronic TTH; intolerance is reduced by starting at 10mg at night and incrementing by 10-25mg each 1-2 weeks usually into the range 50-150mg at night. Sodium valproate 0.6-2.5g daily is an alternative; avoid during pregnancy and use with care in children. • If there is evidence of musculoskeletal problems – physio may be of benefit. If the patient admits to feeling stressed encourage lifestyle changes, relaxation and possibly CBT. Management of Common Headaches seen in GP Assessment requires a detailed history. Exam should include BP, Neuro exam, fundoscopy and neck muscles. If over 50 consider ESR Cluster headache SHOULD BE MANAGED BY A SPECIALIST Frequent, brief, unilateral headaches with autonomic features. The objective in both episodic and chronic CH, not always achievable, is total attack suppression. In most cases, preventive drugs are the mainstay of treatment. Analgesics have no place in treating CH. Acute therapies - Sumatriptan 6 mg subcutaneously is the only proven highly-effective acute treatment - Oxygen 100% at 7 l/min (requires a special mask and regulator) helps some people PROPHYLAXIS Prophylaxis of episodic CH should begin early after the start of a new cluster bout.The following are used by specialists. - Verapamil 240-960 mg/day (Do not take with beta blocker and need ECG to exclude AV block) - Prednisolone 60-80 mg/day for 2-4 days, discontinued by gradual dose reduction - Lithium carbonate 600-1600 mg/day - Ergotamine 2-4 mg/day per rectum, usually omitted every 7th day - Methysergide 1-2mg tds Duration of use of prophylaxis: apart from prednisolone, treatment should be discontinued 2 weeks after full remission. Medication-overuse headache Prevention is ideal, with education the key factor. This type of headache must be excluded in all patients with chronic daily headache. Treatment is withdrawal of the suspected medication(s). Although this will lead initially to worsening headache, with forewarning and explanation it is probably most successfully done abruptly. Within 2-3 weeks, usually, the headache shows signs of improvement. Patients should be reviewed at this time to ensure withdrawal has been achieved. Improvement may be slow but continues for weeks to months. 50-75% of patients revert to their original headache type which may be migraine (usually) or TTH. This headache should be reviewed after 2-3 months and managed appropriately. Most patients require extended support: the relapse rate is around 40% within five years.