Download
1 / 38
380 likes | 540 Views
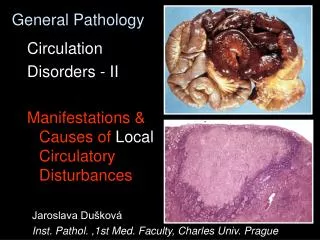
General Pathology. Cellular and Organ Pathology Disorders of Glycogen Degradation. Pathology of Calcification. Jaroslava Dušková Inst. Pathol. ,1st Med. Faculty, Charles Univ. Prague. Disorders of Glycogen Degradation. Pathology of Calcification. Table of contents. Glycogen

E N D
General Pathology Cellular and Organ Pathology Disorders of Glycogen Degradation. Pathology of Calcification. Jaroslava Dušková Inst. Pathol. ,1st Med. Faculty, Charles Univ. Prague
Disorders of Glycogen Degradation. Pathology of Calcification.Table of contents • Glycogen • morphology, function, regulation • pathology states • inborn - glycogenoses • acquired • hyperglycemia – DM I, DM II, MODY • hypoglycemia – insulinoma • hyperglycemia – glucagonoma • glycogen storage in the neoplasms (clear cell kidney ca, seminoma, Ewing sarcoma… • Calcification • dystrophic • metastatic clinical manifestations complications
Glycogen • linear and branched polymer • cca 60 000 - D-glucose molecules • monoparticles (beta) - muscle • complex particles (alpha) - hepatocyte
Main Hormones in Glycogen Metabolism insulin glucagon
The Actions of Insulin on Cells • Increased glycogen synthesis –in liver (and muscle) cells. Reducing high blood glucose levels in diabetes. • Forces adipose tissue to make fats; lack of insulin causes the reverse. • Decreased proteolysis • Decreased lipolysis • Decreased gluconeogenesis • Increased amino acid uptake • Increased potassium uptake • Arterial muscle tone – forces arterial wall muscle to relax, increasing blood flow, especially in micro arteries; lack of insulin reduces flow by allowing these muscles to contract
Glucagon -physiologic effects • increase in blood concentration of glucose. Neurons can not utilize alternative energy sources like fatty acids • Glucagon stimulates breakdown of glycogen stored in the liver. • Glucagon activates hepatic gluconeogenesis. Non-hexose substrates such as amino acids are converted to glucose. • Glucagon also appears to have a minor effect of enhancing lipolysis of triglyceride in adipose tissue.
Control of Glucagon Secretion • Secreted in response to hypoglycemia • Two other conditions : • Elevated blood levels of amino acids, after consumption of a protein-rich meal . Since high blood levels of amino acids also stimulate insulin release both insulin and glucagon are active. • Exercise: not clear whether the actual stimulus is exercise per se, or the accompanying exercise-induced depletion of glucose. • Negative control - glucagon secretion is inhibited by • high levels of blood glucose • insulin • somatostatin
Glycogen Metabolism Diseases • diabetes mellitus type I (& LADA – late autoimmune diabetes of adults) - polygenic HLA-DR 3, 4 • diabetes mellitus type II - polygenic • MODY - more than 10 types described – monogenic • insulinoma • glucagonoma • insulin resistance in : • metabolic syndrome (=obesity, glucose intolerance, hypertension, hyperlipemia… ) • insulin receptor mutations • polycystic ovary syndrome • hypercortisolism…….
Complications of Diabetes glucotoxicity due to: • formation of Advanced Glycation E products • release of pro-inflammatory cytokines and growth factors • generation of ROS (free radicals) in endothelia
Complications of Diabetes • macroangiopathy • microangiopathy • retinopathy • nephropathy • neuropathy • infections….. diabetic gangrene
EnzymesInvolved in Glycogen Metabolism • g.-synthase - brancher • phophorylase kinase - debrancher • g-6-phosphatase • -glucosidase
Glucokinase role in maintenance of glucose homeostasis pancreas – B cell M ATP/ADP glucose – G6P K+ Ca2+ GLUT2 GKB insulin GKA glucose IR GKh GLUT2 glucose G6P glycogen hepatocyte
Storage Diseases Def.: inborn errors of metabolism (mostly single gene abnormality) leading to an enzyme defect with subsequent accumulation of the substrate (& lack of the product) in tissues or organs„thesaurismoses“
Glycogenosis I – von Gierke E defect - gl-6 - phosphatase Organ damage - liver, kidney
Glycogenosis II – Pompe E -defect - alfa1,4-glycosidase Organ damage - heart
Clear Intracellular Vacuoles& adjunct techniques • accumulations of water neg. • lipides SUDAN, OILRED • polysaccharides PAS, A-PAS
Glycogen water soluble easily lost in long lasting water based fixative solutions
Calcification Def.: depositions of Ca (mostly phosphate salts) in tissues or organs Classification: dystrophic metastatic
Calcification - physiology • Matrix vesicles - osteoblasts- nidus calcification • Non collagen proteins - osteopontin, osteonektin, osteokalcin, Gla protein,sialoprotein • Alkalic phosphatase • Phospholipids • Collagen I • Hydroxyapatite
Pathology Conditions with Calcium Deposits Calcification • dystrophic • metastatic Calcinosis • localized • generalized Chondrocalcinosis-pseudogout
Calcification - Microscopy • Basophilic • Von Kossa - Ag impregnation • Alizarine red + • Tetracyclin fluorescence • Polarized light birefringence
Dystrophic Serum Ca level: normal Tissues/Organs status dystrophic changes (necrosis, scar…, low metab. turnover) Metastatic Serum Ca level: Tissues/Organs status normal, local alcalisation (acid secretion - urine, stomach juice, sweat…) Calcification
Dystrophic Serum Ca level: normal Tissues/Organs status dystrophic changes (necrosis, scar…, low metab. turnover) Metastatic Serum Ca level: Tissues/Organs status normal, local alcalisation (acid secretion - urine, stomach juice, sweat…) Calcification
Ca Salts in the Calcified Foci • Ca phophate Ca3(PO4)2 • Ca diphosphate (Ca2P2O7) • Hydroxyapatite (Ca5 (PO4)3.OH
Pathology Conditions with Calcium Deposits Calcification • dystrophic • metastatic Calcinosis • localized • generalized Chondrocalcinosis-pseudogout
Dystrophic Calcification • Frequent • necrotic tissue • connective tissue • vessels • kalkospherites • intracellular calcifiction of lysosoms Less frequent tendon, cartilage, elastics, bas. membranes
Calcinosis Forms - localised generalised Localisation– connective tissue, muscles
Chondrocalcinosis crystal deposit disease (pseudogout) pyrophophate and hydroxyapatite deposits localisation– synovial membrane, cortilage, bone
Calcium pyrophosphate deposition disease(Chondrocalcinosis, pseudogout) • Clinic: may simulate different diseases • Arthroscopy - chalky white deposits • Tophaceus deposits with crystalline aggregates • Crystals stain with von Kossa technique • Foreign body type multinucleated giant cell reaction • Deposits are in synovium, cartilage, bone
Vitamin D3 (1,25(OH)2D3) is a Hormone • Vitamin D3 is not politically correct. • It discriminates depending where you live, the further you live from the equator the less sun exposure consequently the lower your Vitamin D3 level. • It discriminates against the elderly, as you age your skin loses up to 75% of its ability to make Vitamin D3. • It discriminates against the obese. They have lower levels of Vitamin D3, due to the fact it is oil soluble, that it builds up in the fat tissue. • It discriminates against skin color a dark complected person needs more sun exposure to produce their Vitamin D3 than a fair skinned person. • It also discriminates against a person who does as they are told. It has been reported the incident of breast cancers have increased 40% in Australia due to Vitamin D3 deficiency caused by sunscreen use.
Metastatic calcification - causes • PTH secretion adenoma, carcinoma • destruction of bone – leukemia, myeloma, metastases, Paget (polyostotic) • vitamin D intoxication • renal failure – phophate retention - secondary hyperparathyreosis - PTH
Pathology Conditions with Calcium Deposits Calcification • dystrophic • metastatic Calcinosis • localized • generalized Chondrocalcinosis–pseudogout Calciphylaxix – extensive microvascular calcification and occlusion / thrombosis
Almafragi A, Vandorpe J, Dujardin K.Calciphylaxis in a cardiac patient without renal disease.Acta Cardiol. 2009 Feb;64(1):91-3. Calciphylaxis is a rare complication that occurs in 1% of patients with end-stage renal disease (ESRD) each year. Extensive microvascular calcification and occlusion/thrombosis lead to violaceous skin lesions, which progress to nonhealing ulcers with secondary infection, often leading to sepsis and death. The lower extremities are predominantly involved (roughly 90% of patients). Although most calciphylaxis patients have abnormalities of the calcium-phosphate axis or elevated levels of parathyroid hormone, these abnormalities do not appear to be fundamental to the pathophysiology of the disorder. We report on a case of histologically proven calciphylaxis in a 54-year-old woman with normal renal function and normal calcium-parathyroid homeostasis. She had a history of alcoholic cardiomyopathy, and was treated with warfarin anticoagulation. She has been successfully treated with antibiotics, i.v. biophosphonates and intensive local wound care. We recorded a complete wound healing in contrast to what is reported in other series.
Calciphylaxis reported in: • hypoalbuminemia • malignant neoplasm • systemic corticosteroid use • anticoagulation with warfarin • chemotherapy • systemic inflammation • hepatic cirrhosis • obesity • rapid weight loss, and • infection….