Download
1 / 14
150 likes | 368 Views
Percutaneous Coronary Intervention Versus Conservative Therapy in Nonacute Coronary Artery Disease: A Meta-Analysis. Demosthenes G. Katritsis, MD, PhD; John P.A. Ioannidis, MD. Published in Circulation 2005. PCI vs. Conservative Therapy: Background.

E N D
Percutaneous Coronary Intervention Versus Conservative Therapy in Nonacute Coronary Artery Disease: A Meta-Analysis Demosthenes G. Katritsis, MD, PhD; John P.A. Ioannidis, MD Published in Circulation 2005
PCI vs. Conservative Therapy: Background • The potential benefits of percutaneous coronary intervention (PCI) in the management of stable patients with coronary artery disease (CAD) in nonacute settings have been debated for more than a decade. • Although PCI has been shown to improve symptoms compared with conservative treatment in patients with stable CAD, there is limited evidence on the effect of PCI with regards to death, myocardial infarction (MI), and subsequent revascularization. • The results of a meta-analysis from 11 studies in patients with angiographically documented coronary artery stenosis in nonacute CAD settings are reported. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Study Design 2950 patients from randomized trials comparing coronary revascularization by PCI versus conservative medical therapy for treatment of patients with CAD documented by angiographic evidence of stenosis of 1 or more coronary vessels Meta-Analysis Mean age range 53-61 years, predominantly or exclusively male population, mean follow-up in 5 trials (with 1790 patients) exceeded 2 years, more limited follow-up data available in other 6 trials (1160 patients), no trial used DES Conservative Therapy n=1474 PCI n=1476 • Primary Endpoint: Death, Cardiac Death or nonfatal MI, CABG, and PCI during follow-up (in the target vessel or other vessel/segment). - All data used pertained to the longest follow-up available per outcome from each study Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Primary Endpoint • There were a total of 196 deaths, 235 patients had cardiac death or MI, 153 patients had nonfatal MIs, 215 patients underwent CABG, and 462 had PCI during follow-up. • Despite some differences, there was no statistically significant between-study heterogeneity for death, cardiac death or MI, nonfatal MI, and need for CABG; thus, random and fixed effects estimates were very similar for these outcomes. Number events per treatment group (# patients) # patients Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Risk Ratio for Death • There was large between-study heterogeneity in the risk ratios for PCI during follow-up. • There was no difference shown in the summary estimates between PCI and the conservative group in the mortality risk. • The 95% confidence intervals excluded relative risk differences of 28%. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
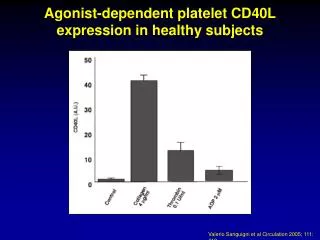
PCI vs. Conservative Therapy: Risk Ratio for Cardiac Death or MI • There was a trend for more cardiac deaths or MIs (Figure B), especially nonfatal MIs (Figure C) in patients who underwent PCI. • The point estimate suggests approximately a 30% increase in the relative risk of nonfatal MI with PCI. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Risk Ratio for CABG • Between the two compared treatment strategies, there was no difference in the need for CABG. • The 95% confidence intervals also excluded differences in the relative risk exceeding 20% in favor of PCI and 33% in favor of conservative treatment. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Risk Ratio for PCI during follow-up • Although there was no overall difference in the risk for PCI during follow-up, the random effects 95% confidence intervals were more substantial given the considerable variability between study heterogeneity. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Sub Group Analysis • Subgroup analyses showed that availability of stents did not make a substantial difference for any of the 5 end points. • In trials with follow-up exceeding 2 years, there were no differences between PCI and conservative treatments, with RR estimates very close to 1.00 for all outcomes. • Trials with more limited follow-up suggested an increase in deaths, MI, and nonfatal MI in PCI-treated patients, and the difference reached formal statistical significance for cardiac death or MI, with almost a doubling of risk conferred by PCI; however, the CIs overlapped with the results from longer term trials. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Limitations • Data were not available consistently across these trials to separate procedure based infarctions from subsequent MI. • It is unlikely that myocardial enzymes were routinely checked after PCI so that risk of post PCI MI may have been underestimated. • Also, minor procedure-related infarctions without definitive ECG changes may have been largely underreported in the PCI arms. • Several of these trials were conducted in the time period before the routine use of stents in clinical practice. • The disease background of the patients included was different across trials. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Limitations (cont.) • Additionally, patient populations differed across trials with respect to intensity of angina symptoms, functional demonstration of ischemia, and angiographic extent of CAD. • The included trials did not routinely use the full spectrum of conservative interventions currently available for CAD management. • Overall the varying and potentially suboptimal medical management across trials is a limitation of the meta-analysis; however, one would expect better outcomes if the management were optimized. • Lastly, the present meta-analysis did not consider the option of CABG in patients with stable chronic CAD and preserved LV function. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Summary • Compared with conservative therapy, PCI does not decrease mortality or the risk of MI during follow-up in patients with chronic CAD. • A trend for increased risk of MI in patients undergoing PCI was observed, which may reflect the risk inherent in the invasive procedure itself. • Although early literature suggests that PCI may cause an increased need for CABG, there was no evidence for an increased need for CABG in the PCI group compared with the conservative strategy group. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912
PCI vs. Conservative Therapy: Summary (cont.) • Similarly, there was no difference in the risk of requiring PCI during follow-up with interventional versus conservative therapy; however, there was considerable variability in this outcome across trials. One possible explanation for this heterogeneity is that although indications for CABG are relatively clear-cut, indications for PCI are more subjective, meaning that different investigators and sites may have had different biases toward the use of PCI during follow-up based on whether or not it was used prior.
PCI vs. Conservative Therapy: Summary (cont.) • Importantly, even when analyses were limited to studies that used stents, this meta-analysis found no evidence of superiority for the PCI strategy. • In conclusion, in the absence of acute coronary syndromes, for patients with chronic CAD and good LV function, PCI does not confer any clear benefit in terms of long-term hard clinical outcomes compared with conservative medical therapy. • Randomized trials in the modern era of pharmacotherapy and new device interventions is lacking. Katritsis DG & Ioannidis J.P.A., Circulation 2005; 111:2906-2912