Download
1 / 1
10 likes | 149 Views
Sexual dysfunctions in HIV-positive women. Sonnenberg-Schwan U 1 , Kästner R 2 , Müller M 2 , Gingelmaier A 2 , Friese K 2. 2 Frauenklinik der LMU München - Innenstadt. 1 Section ALL AROUND WOMEN special, DAIG e.V. Introduction

E N D
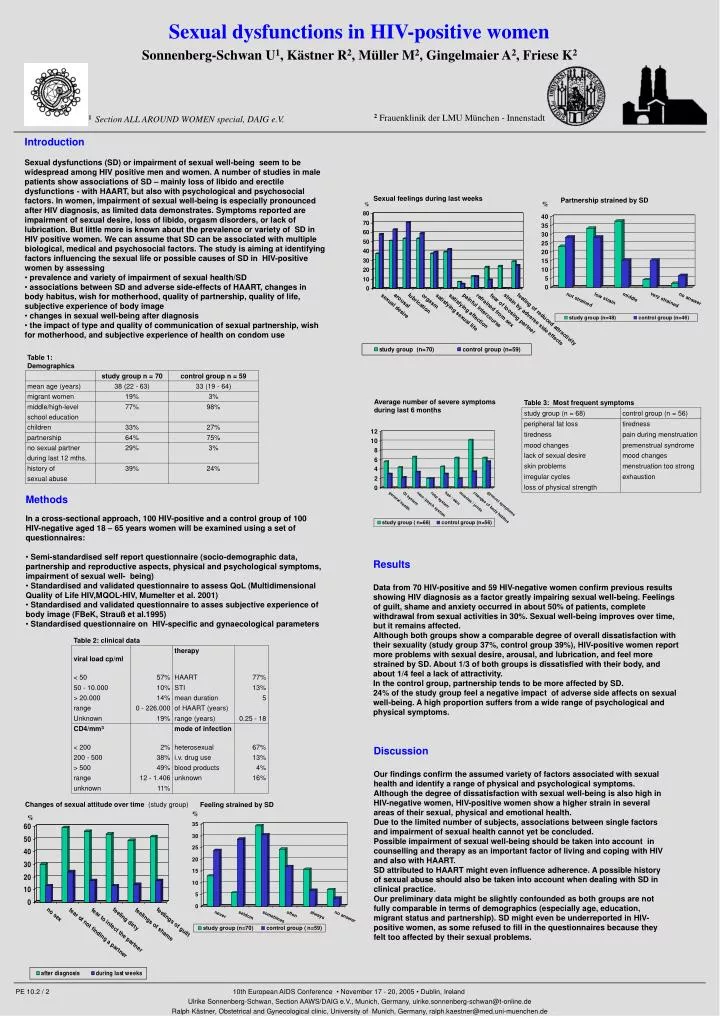
Sexual dysfunctions in HIV-positive women Sonnenberg-Schwan U1, Kästner R2, Müller M2, Gingelmaier A2, Friese K2 2Frauenklinik der LMU München - Innenstadt 1 Section ALL AROUND WOMEN special, DAIG e.V. • Introduction • Sexual dysfunctions (SD) or impairment of sexual well-being seem to be widespread among HIV positive men and women. A number of studies in male patients show associations of SD – mainly loss of libido and erectile dysfunctions - with HAART, but also with psychological and psychosocial factors. In women, impairment of sexual well-being is especially pronounced after HIV diagnosis, as limited data demonstrates. Symptoms reported are impairment of sexual desire, loss of libido, orgasm disorders, or lack of lubrication. But little more is known about the prevalence or variety of SD in HIV positive women. We can assume that SD can be associated with multiple biological, medical and psychosocial factors. The study is aiming at identifying factors influencing the sexual life or possible causes of SD in HIV-positive women by assessing • prevalence and variety of impairment of sexual health/SD • associations between SD and adverse side-effects of HAART, changes in body habitus, wish for motherhood, quality of partnership, quality of life, subjective experience of body image • changes in sexual well-being after diagnosis • the impact of type and quality of communication of sexual partnership, wish for motherhood, and subjective experience of health on condom use Sexual feelings during last weeks Partnership strained by SD % % Average number of severe symptoms during last 6 months • Methods • In a cross-sectional approach, 100 HIV-positive and a control group of 100 HIV-negative aged 18 – 65 years women will be examined using a set of questionnaires: • Semi-standardised self report questionnaire (socio-demographic data, partnership and reproductive aspects, physical and psychological symptoms, impairment of sexual well- being) • Standardised and validated questionnaire to assess QoL (Multidimensional Quality of Life HIV,MQOL-HIV, Mumelter et al. 2001) • Standardised and validated questionnaire to asses subjective experience of body image (FBeK, Strauß et al.1995) • Standardised questionnaire on HIV-specific and gynaecological parameters Results Data from 70 HIV-positive and 59 HIV-negative women confirm previous results showing HIV diagnosis as a factor greatly impairing sexual well-being. Feelings of guilt, shame and anxiety occurred in about 50% of patients, complete withdrawal from sexual activities in 30%. Sexual well-being improves over time, but it remains affected. Although both groups show a comparable degree of overall dissatisfaction with their sexuality (study group 37%, control group 39%), HIV-positive women report more problems with sexual desire, arousal, and lubrication, and feel more strained by SD. About 1/3 of both groups is dissatisfied with their body, and about 1/4 feel a lack of attractivity. In the control group, partnership tends to be more affected by SD. 24% of the study group feel a negative impact of adverse side affects on sexual well-being. A high proportion suffers from a wide range of psychological and physical symptoms. Discussion Our findings confirm the assumed variety of factors associated with sexual health and identify a range of physical and psychological symptoms. Although the degree of dissatisfaction with sexual well-being is also high in HIV-negative women, HIV-positive women show a higher strain in several areas of their sexual, physical and emotional health. Due to the limited number of subjects, associations between single factors and impairment of sexual health cannot yet be concluded. Possible impairment of sexual well-being should be taken into account in counselling and therapy as an important factor of living and coping with HIV and also with HAART. SD attributed to HAART might even influence adherence. A possible history of sexual abuse should also be taken into account when dealing with SD in clinical practice. Our preliminary data might be slightly confounded as both groups are not fully comparable in terms of demographics (especially age, education, migrant status and partnership). SD might even be underreported in HIV-positive women, as some refused to fill in the questionnaires because they felt too affected by their sexual problems. Changes of sexual attitude over time (study group) Feeling strained by SD % % PE 10.2 / 2 10th European AIDS Conference • November 17 - 20, 2005 • Dublin, Ireland Ulrike Sonnenberg-Schwan, Section AAWS/DAIG e.V., Munich, Germany, ulrike.sonnenberg-schwan@t-online.de Ralph Kästner, Obstetrical and Gynecological clinic, University of Munich, Germany, ralph.kaestner@med.uni-muenchen.de