Download

1 / 41
410 likes | 649 Views
LEISHMANIA. Classification Leishmania parasites for humans have been Classified into 2 broad groups: A) Causing Visceral Leishmaniasis (VL) The L.donovani complex infecting internal organs (Liver, Spleen, Bone Marrow) causing Visceral

E N D
Classification Leishmania parasites for humans have been Classified into 2 broad groups: A) Causing Visceral Leishmaniasis (VL) The L.donovani complex infecting internal organs (Liver, Spleen, Bone Marrow) causing Visceral Leishmaniasis B) Causing Cutaneous & / or Muco cutaneous Leishmaniasis (CL) 1. L.tropica – (Old World CL) 2. L.mexicana complex, L.braziliensis complex – (New world or American CL)
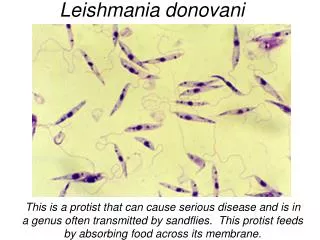
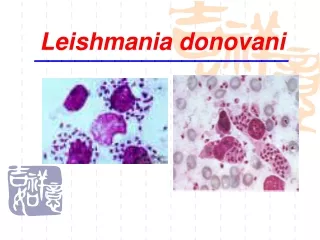
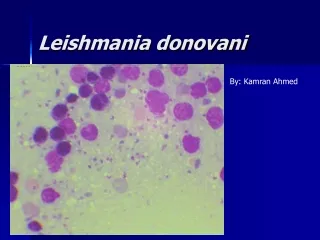
Morphology: The parasite exists in 2 stages • Amastigote stage (formerly called Leishmanial forms) • - Occurs in Man • 2) Promastigote Stage (formerly called Leptomonad form) • - Occurs in • - Gut of Insect (Sand Fly) • - Artificial culture
Amastigote Stage : (Aflagellate Stage) Parasite → Resides in cells of RE system of vertebrate hosts (Man, Dog & Hamster) Characteristics: • Shape & Size-Round/Oval, 2 – 4 µm along longitudinal axis. • Nucleus- 1µm – diameter, Oval/Round in shape. • Kinetoplast- Situated at right angles to Nucleus contains DNA containing body & a mitochondrial structure. • Axoneme- Delicate filament extending from kinetoplast to margin of body. • Vacuole- Clear, unstained space along Axoneme.
Promastigote Stage : Flagellar Stage Parasite → Cultures & Insect vectors (Sand Flies) Characteristics: • Size & Shape- • Early ones- Short Oval/Pear shaped bodies, 5 – 10µm in length and 2 – 3µm in breadth. • Fully developed- Long, slender spindle shaped bodies, 5 – 20µm in length and 1-2µm in breadth • Kinetoplast - Transversely near anterior end. • Vacuole- Eosinophilic, in front of kinetoplast over which root of flagellum runs. • Flagellum-May be of same length as body or longer. • Nucleus- Central
Cultivation • Cultured in a medium composed of 2 parts of Salt Agar & 1 part defibrinated Rabbit’s Blood. • Material for culture → inoculated at 22ºC-24ºC • Presence of Ascorbic acid & hematin favours growth • Medium- introduced by Navy & Neal, later modified by Nicolle. So named NNN medium • Temp: 37ºC for 32 days • Susceptible Animal: Dog
Reservoirs of Infection Dog in – Mediterranean areas China Brazil Method of Transmission Man to Man → Sand Fly of genera Phlebotomus & Lutzomyia Leishmaniasis does not exist in India hence in India man is only source of infection
KALA - AZAR Visceral leishmaniasis was 1st characterised in India, where it was known under the names •Kala-Azar (Black Sickness) •Dum Dum fence •Burdwan fever •Tropical Splenomegaly Incubation Period: 3 – 6 months.
CLINICAL FEATURES • Pyrexia • Splenic Enlargement • Liver Enlargement • Lymphadenopathy
In African Kala-Azar warty eruption on the Skin & Muco cutaneous Lesion may appear • If left untreated, 75 – 90 % patients die within 2 yrs with complications – Amoebic/Bacillary dysentry,pulmonary TB,Pneumonia,Cancrum oris.
Lab diagnosis of Kala Azar Direct evidence Indirect evidence Demonstration of L.donovani Biopsy Peripheral Blood Blood Culture Material obtained by • Amastigote form • Promastigote Splenic puncture Sternal/Iliac crest Puncture(marrow) Lymph node Biopsy Aldehyde test Antimony test Complement Fixation test
Leishmanin test :Killed culture injected intradermally + ve reaction produced in Kala azar cases 6 – 8 wks after recovery & represents a delayed hypersensitivity reaction accompanied by CMI Alders test : Development of promastigote of Leishmania in Locke’s serum agar can be inhibited by a specific immune serum but can take place in heterologous serum
PROPHYLAXIS • Attack on parasite • Attack on the vector • Personal prophylaxis
DERMAL LEISHMANOID (POST KALA AZAR DERMAL LEISHMANIASIS) A type of non ulcerative cutaneous lesion prevalent in endemic areas of Kala azar in India (Bengal, Madras & Assam) Clinical manifestations - Deep pigmented macules - Erythematous patches (Butterfly erythema) - Yellow pink nodules Diagnosis:Biopsy
L.Tropica [parasite causing Cutaneous Leishmaniasis] Geographical Distribution Mediterranean Central & Western India (drier pats) Central Africa Persia Habitat: Inside Clasmatocytes (cells of RE sys) of skin Morphology: Amastigote form → in Man Promastigote form → in Cultures & Sandflies
Cultivation: in NNN -Novy, Mac.Neal,Nicolle medium • Susceptible Animals: In Mice, intraperitoneal inoculation produces Visceral infection • Pathology • Nature of lesion is characterised by a chronic infective Granuloma with fibrosis. • In early stage, proliferation of the cells of RE system (Monocytes/Macrophages) forms the primary reaction, inside which parasites are found in large numbers • Later, round cell infiltration associated with a marked reduction in number of parasites & development of a delayed hypersensitive skin reaction (Leishmanin reaction) occur
CLINICAL FEATURES • Oriental Sore (tropical sore) / Delhi boil (slow healing open ulcer/sore) • It ulcerates having clean cut margin with a railed indurated edge, surrounded by red areola • Core has tendency to heal spontaneously but slowly, taking 6 months. The ulcer is filled up by granulomatous tissues, a depressed white scar is often left
LAB DIAGNOSIS • Leishmanin/Skin test is positive in cases of Oriental sore • Prophylaxis • Elimination of reservoir hosts • Control of Sandflies • Individual protection from Sandfly bite • Prophylactic immunisation with a culture of L.tropica
CUTANEOUS LEISHMANIASIS New World Disease Common in Algeria, Iran, Iraq, Saudi Arabia, Syria, Peru, Brazil, Afganistan Etiological agents: L.mexicana complex Old World Disease L.Tropica
MUCOSAL LEISHMANIASIS • Rare • Infection of Naso-oropharyngeal mucosa • Clinical Manifestations • Persistant unusual nasal symptoms (Epistaxis) with Erythema, Edema of Nasal mucosa • ↓ • Ulceration • ↓ • Naso-oropharyngeal destruction
INTRODUCTION • These type of flagellates live in the blood or tissue of man or other animals.
GENERIC CHARACTER • These exits as trypomastigotes in vertebrate hosts (man or animals). • They pass their life cycle in two hosts : • Vertebrate • Insect • While developing inside the insect host, they pass through the stages of amastigote , promastigote, epimastigote & metacyclic form of trypomastigote. • Multiplication can takes place in any of these developmental stages. • Transmission is effected from one vertebrate to another by blood – sucking insects.
CLASSIFICATION • It causes African trypanosomiasis in man & nagna in domestic animals. TRYPANOSOMA BRUCEI
HABITAT • T. brucei is essentially a parasite of connective tissues, where it multiplies readily. It invades the regional lymph nodes through the lymphatics & also invades the blood stream causing Parasitaemia. It finally localises in the brain. MORPHOLOGY : T. brucei exits in vertebrate host as a trypomastigoteform. • It is an elogated rather flattened spindle - shaped organism with a blunted posterior end & a finely pointed anterior end. • The nucleus is large, oval & central in position • The kinetoplast is small & present in the posterior end of the body. • The flagellum starts near the posterior end, curves around the body & continues beyond the anterior end as a free flagellum.
STAINING REACTION • When stained with Leishman or some other modifications of romanowsky stain: a) The cytoplasm & the undulating membrane appear pale blue b) The nucleus is reddish purple in colour c) The kinetoplast & the flagellum dark red. CULTIVATION: It has been cultivated in a medium of Ringer’s solution with sodium chloride, Tyrode’s solution & citrated human blood. ANIMAL INOCULATION • Laboratory animals like mice, rats and guiuea pigs are generally inoculated for demonstrating the tryopmastigotes when they are scanty or difficult to find in the peripheral blood of the man.
LIFE CYCLE • T. brucei passes its life cycle in two different hosts: • The vertebrate hosts are man, and domestic amimals. • The insect hosts are several species of the tsetse fly.
TRANSMITTING AGENTS & RESERVOIR OF INFECTION • The animal strain of T. brucei is transmitted by Glossinamorsitans amongst the wild game and domestic animals. PATHOGENESIS 1) Mode of infection: By the bite of the infective tsetse fly Glossina. Some trypomastigotes may enter the blood stream but majority remains entangled in the tissue spaces. The presence of trypomastigotes in the tissue spaces excites host’s response in two ways: • By producing large amount of non-specific immunoglobulin which are not able sensitising the antigen. • By the action of macrophages. The neutrophils take little interest in the defence.
2) Pathogenic lesion: • There is severe damage of the perivascular connective tissue. • The lesions are found mainly in the lymph nodes & central nervous system. Laboratory diagnosis: • This is established y demonstrating the following: • Peripheral blood • Bone marrow obtained by sternal puncture • Juice aspirated from the swollen lymph nodes • The cerebrospinal fluid obtained by lumbar puncture.
TRYPANOSOMA CRUZI • GEOGRAPHICAL DISTRIBUTION: Central & South America. • HABITAT: A parasite of musculra & nervous tissue & also of the reticular endothelial system.
MORPHOLOGY Two main morphological types are found in human host: • A) Trypomastigote form: In dried and stained film it appaers to be C or U shaped. • It measures 20 micrometer in length,has central nucleus and a large, oval kinetoplast situated at the posterior end. • B) Amastigote form: The amastigote forms are round or oval bodies, measuring 2 to 4 micrometer in diameter, having nucleus & a kinetoplast.
STAINING REACTION • When stained with Leishman or some other modifications of romanowsky stain: a) The cytoplasm & the undulating membrane appear pale blue b) The nucleus is reddish purple in colour c) The kinetoplast & the flagellum dark red.
IMMUNOLOGY • Serum antibodies develop in T. cruzi infection but as the parasite continues to grow, so they are not exposed to the action of these antibodies.
RESERVOIR HOSTS • These are Armadillos & opossum. • Man is the secondary host. LABORATORY DIAGNOSIS • By microscopic examination of a stained blood film. • By inoculating a guinea pig with patient’s blood. • By a specific complement fixation test with antigen obtained from culture of T. cruzi.