Download

1 / 16
260 likes | 532 Views
Isolated heart perfusion Langendorff-model. Kåre-Olav Stensløkken Division of Physiology Department of Molecular Medicine. Oscar Langendorff 1853-1908 Isolated heart model Published in 1895 (Pflugers Arch). Aims of this talk:. Explain the principle of isolated heart perfusion

E N D
Isolated heart perfusionLangendorff-model Kåre-Olav Stensløkken Division of Physiology Department of Molecular Medicine
Oscar Langendorff 1853-1908 Isolated heart model Published in 1895 (Pflugers Arch)
Aims of this talk: • Explain the principle of isolated heart perfusion • Strengths and limitations of the model
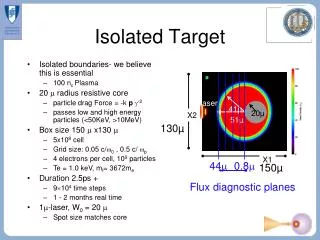
Principle of isolated heart perfusion: • the heart is rapidly exsiced and placed on ice-cold buffer • aorta is disected free and cannulated • the heart is mounted in a perfusionapparatus with oxygenated buffer 37°C • retrograde perfusion: buffer comes from the aorta into the coronary arteries (the cannula is placed above intact aortic valves) • modification from Oscar Langendorff: A balloon is inserted into the left ventricle to register pressure and heart frequence
Schematic presentation of the perfusion apparatus Oxygenated Krebs Henseleit buffer (95%02, 5%CO2) Either constant perfusion pressure or constant flow AD-converter PC - ECG - Pressures - Coronary flow External water bath 37°C Isolated heart
Intraventricular balloon • Retrograde perfusion: buffer from aorta to coronary arteries (cannula placed above intact valve) • Modified from Oscar Langendorff: balloon is placed in left ventricle to measure function
End points Stab Ischemia Reperfusion Perfusion Pressure Coronary Flow Infarct size Myocardial necrosis after ischemia Triphenyl tetrazolium chloride (TTC) detects lactate dehydrogenase activity in viable tissue which stains red, while necrotic remains unstained (white) • Technically challenging to delineate borderzones in small hearts • OBS artefacts due to cutting and freezing
End points Stab Ischemia Reperfusion Coronary Flow Perfusion Pressure Left ventricular end diastolic pressure
End points Stab Ischemia Reperfusion Coronary Flow Perfusion Pressure • Left ventricular developped pressure • Left ventricular systolic pressure • Heart rate • Contractility • Coronary effeluent • Tissue for molecular analysis
Advantages: Well characterized in the litterature • Large freedom of experimental design • Requires only one researcher • Easy to learn (not mice) • Cheap • Supplemental studies are easy to perform (collection of effluents and hearts/other organs/blood) • Gives a good evaluation of heart function without confounding affects of preload and afterload • Contrallable model and reproducible results
Disadvantages: • Denervated heart without influence of hormones and circulating blood components • Passivly perfused heart (non-working) • Not good for finer evaluations of coronary flow • Infarct size may be hard to estimate exactly in mice • In models of global ischemia there is a large increase of end-diastolic pressure • ”Molecular state” will be different than in-vivo due to handling stress
The «molecular state» will change from in-vivo P38-MAPK phosphorylation over time in the Langendorff perfused heart Bliksøen et al. unpublished
Langendorff in mice: Fluctuations 70 mmHg LV Pressure min Perfusion Pressure Coronary Flow min 55 mmHg LV Pressure
Summary The Langendorff-model can give a good overview of organ function with specific interventions or genetic modifications The findings can not be directly extrapolated to the in vivo situation Mice challenge us with species-specific regulation of normal physiology