Download
1 / 18
180 likes | 269 Views
SUPRATECH MICROPATH LABORATORY & RESEARCH INSTITUTE. Case -7. Dr. BHAVANA MEHTA Consultant pathologist Supratech micropath laboratory and research institute, Ahmedabad. Clinical details. 38 yrs, male Renal transplant- 5 yrs back On cyclosporin ,Azoran, steroids

E N D
SUPRATECH MICROPATH LABORATORY & RESEARCH INSTITUTE Case -7 Dr. BHAVANA MEHTA Consultant pathologist Supratech micropath laboratory and research institute, Ahmedabad
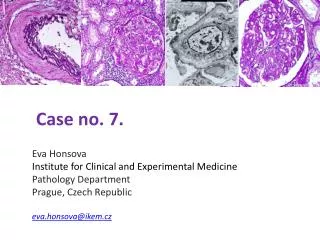
Clinical details • 38 yrs, male • Renal transplant-5 yrs back • On cyclosporin ,Azoran, steroids • S cr- gradually increased upto 3.0, urine protein++ • Renal biopsy done
Provisional Diagnosis Post transplant myeloma cast nephropathy
Why cast nephropathy in post Tx • Allograft nephropathy • ARF • Drug related cast
Pathogenesis of myeloma cast nephropathy • Common in multiple myeloma • Due to over production and precipitation of light chain • Resistant to degradation due to structural changes • Increased urinary calcium due to hypercalcemia • Acute renal failure due to other disease (volume depletion • Drug related –loop diuretics by increasing luminal NaCl • Radiocontrast media interacting with light chains
What are myeloma casts? • Precipitated light chains in distal and collecting tubules +other filtered proteins+Tamm-Horsfall mucoprotein which a protein normally secreted by cells of thick ascending loop of Henle and constitute matrix of all urinary casts • Disruption of BM of tubule-leakage-cellular reaction
Other disease with myeloma casts • Acinar cell carcinoma, pancreas • Waldenstrom macroglobulinemia • B cell lymphomas • Thyroid carcinoma
History retrieved H/o basic disease-Myeloma kidney diagnosed in 2001 Urine-Bence John’s protein present Protein electrophoresis –M band present
Final diagnosis • Relapse of myeloma cast nephropathy, renal graft. • Donor-sister • No family history • Post transplant period-no problem till 5 yrs
Post Tx myeloma cast nephropathy • Usually Tx not considered in myeloma pt. • Becasuse of risk of recurrence & relapse • If in remission for 1 yr, considered for Tx • Usually recurrence noted within 2 yrs
Post Tx myeloma cast nephropathy • One case reported in early transplant period associated with thrombotic microangiopathy • Upto 10 cases of MM and few with AL amyloidosis received Tx- more post Tx mortality • With recent treatments available for MM- Better post Transplant period
Reasons to present this case Young Patient to have MM No Bone marrow involvement Intraabdominal mass-reported as Multiple myeloma Late graft dysfunction-5 yrs Presently on Thalidomide and doing well patient