Download
1 / 51
520 likes | 771 Views
Exercise Prescription for Health Irish Association of Cardiac Rehabilitation. Joseph Cummiskey MD Dean FSEM, RCSI and RCPI President EFSMA 11 th November, 2013. The program this evening. Introduction: Why exercise is good?

E N D
Exercise Prescription for HealthIrish Association of Cardiac Rehabilitation Joseph Cummiskey MD Dean FSEM, RCSI and RCPI President EFSMA 11th November, 2013
The program this evening • Introduction: Why exercise is good? • The big question which the FSEM faces “how much physician input?” • Exercise talk: EPH, an initiative of EFSMA; what is involved? ICGP
IntroductionWhy exercise is good Part 1. No conflicts of interest
The ethics of not prescribing exercise:Is it negligence? • Large studies from Europe and the USA have shown that low cardio-respiratory fitness is the single biggest risk factor for all-cause mortality. • The importance of sports medicine, in particular the benefits of physical activity in non-communicable disease prevention and chronic disease management, should be incorporated into the core under and post graduate teaching
Exercise Physicians and other health professionals can contribute substantially to patients' adoption of exercise behaviours, just as they have provided smoking cessation advice and contribute to smoking reduction in many countries. A straightforward but influential step forward would be measurement of the exercise as the 5th vital sign in every consultation. Patients ought to report how many minutes of physical activity they undertake in an average day and how many days a week such activity takes place.
Nothing about exercise is new As old as history itself Hippocrates 5th century “if one exercised they become more healthy, well-developed and age more slowly” Herodotus 5th century BC. The father of histories “If we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health”. Plato: 5th BC. “Lack of activity destroys the good condition of every human being, while movement and methodical physical exercise save it and preserve it”.
There has been an Acceleration in knowledge technologyabout exercise physiology • Occurred in 1968 after Karl Wasserman, Brian Whipp and Antonius Van Kessel published their paper on breath by breath analysis during exercise. This microprocessor now forms the basis for all clinical C-P ex tests machines. • This was supplemented by the introduction of the Hewlett Packard ear oximeter in 1970. • At last we had non-invasive measurements of heart (rate and rhythm) and lung (air volumn, oxygen utilisation, carbon dioxide production, respiratory rate, respiratory exchange ratio, prediction of anaerobic threshold) and their ratios, that could be done during exercise.
Why? • Why is it if exercise is good for you we all do not exercise enough. • The answer lies in religion; all religions knew from the start of their religion that “We must be constantly reminded of what we believe in”. • If patients and the general public are not constantly reminded to exercise they will not do so. • This is where the physician plays a role
The House of Lords, UK, Science and Technology Committee • The above group launched a new short inquiry into sports and exercise science and medicine after the London Olympics in 2012. • Commenting, Lord Krebs, Chairman of the Committee, said: “There is an ever-growing body of evidence showing that increasing the amount of exercise people take can be of huge benefit in treating a wide range of chronic conditions. However, we are not convinced that health professionals currently have the skills or support to prescribe appropriate training regimes for their patients” (My, as President, emphasis).
What does that tell you? • Doctors need to be more knowledgeable about exercise and how to prescribe it. • They must know what to tell their patients • They must do PPE which include an ECG and possibly a CP ex test in some patients • They must follow up after a prescription has been completed
Risks of exercise prescription is the reason exercise is not medicine for all Sudden cardiac death Exercise related cardiac events An important point is that SCA is seven fold more common in participants who do not have a pre-participation assessment. A different etiology for SCA appears with PPE ECG (Italy v USA) Exercise induced asthma Exercise induced hypoxemia Hypoglycemia of exercise
(Corrado et al. NEJM 1998) Anomalous c.a. origin 12% ARVD 23% Premature CAD 18% Anomalous c.a. origin 12% ARVD 3% HCM 2% athletes <35 yrs Atherosclerotic c.a. disease 2% HCM 36% (Maron et al. JAMA 1996)
The Big Question • “How involved should the doctor be in the exercise management of health and disease”. • I cannot see the case for not wanting any medical input at all. This is the way it has been for years in most countries • The positive impact of Medical input at start and follow up I believe is the next step to getting the most from an exercise prescription.
The European Federation of Sport Medicine Associations approach to exercise Exercise Prescription for Health (EPH) Part 2
European Federation of Sports Medicine Associations (EFSMA) Over 200 man hours of discussion on EPH and EIM in 2012 Contained representatives from 10 of the 41 EFSMA affiliated countries (included Italy, Germany, Austria, Belgium, Turkey, France, Ireland, Norway, Portugal and Cyprus) Listened to all arguments for and against PPE Title of the initiative Analysed what was being used in various countries by written surveys and word of mouth Planted the flag for EPH in Rome in 9.2012 Follow up in Athens 3.2013 Follow up in Dublin 23.4.2013 Major launch in Strasbourg 9.2013 to 35 European countries Sweden has requested a major role.
EPH and why it is the correct title • Exercise and/or physical activity are essential in a title. • Prescription suggests that a thoughtful note is written by a doctor for a certain course of action • Heath was always the term used by the ancient Greeks as distinct from Medicine which implies a universal beneficial outcome
“Exercise Is Medicine” and why it is a misnomer • The title EIM is an oxymoron (a figure of speech where apparently contradictory terms appear in conjunction) • If exercise causes death or disease can we call it a medicine? • Exercise induced asthma or bronchospasm occurs in 3/100 athletes • 3/100,000 people die from Sudden cardiac arrest syndrome usually during or after exercise • Exercise has side effects and therefore should be treated like a drug • EIM-USA is a dumbing down of the science of exercise. • It is written by sport scientists and sports medicine doctors mainly for sport scientists to be the major prescribers.
Exercise is MedicineTM (EIM) • It retains fiscal and legal control (68 page Memorandum of Understanding) to be signed before you can use the trade mark EIM). • If EFSMA were to try to match this with a contract the estimate for legal expenses was said to be €50,000 euro. • EIM has only a history and family history as the preparticipation assessment. • It has a lot of psychology, poor clinical standards and no science.
EIM • It is a marketing tool for exercise. • EIM is a global trademark only in the USA. • It insists all printing is done in Indianapolis. • It would take a maximum of 15% of all sponsors funds raised for EIM in your country • It has sport scientists deciding the exercise and sports medicine doctors signing the prescription and taking the responsibility • It would be politically a disaster for European Sport Medicine and that is why we believe EFSMA were never contacted directly by EIM
Other European groups • ECSS (European College of Sport Science) want to be involved in the research of exercise • HEPA (Health-Enhancing Physical Activity) EU / C of E do not want to do the medical hands on part of exercise but rather write the guidelines. • EIM-E (Exercise is Medicine-Europe) only requires a clinical and family history. The end point is a feel good factor. • NICE (National Institute of Health and Care Excellence) UK: PA brief advice for adults in primary care
Who supports EPH? • European Federation of Sport Medicine Associations (EFSMA) • International Federation of Sports Medicine (FIMS) • European Olympic Committee, Medical Commission (EOC, MC) • Council of Europe (C of E) • European Academy of Science and the Arts (EASA) • European Union Medical Specialities (UEMS, MJC, SM) • Medica, a Medical conference organiser, Dusseldorf
President of the Eur Academy of Science and the Arts, Prof Unger • EFSMA FIMS Academy FIMS UEMS EFSMA Medica
Council of EuropeExercise in Europe 2007 • The concept of Exercise as a Health tool they said “was becoming increasingly important”. • They also stated that “SEM Physicians are able to • evaluate medical patients co-morbidities, • perform exercise testing and • provide an exercise prescription, together with • a motivational programme and exercise classes”. • BUT Between 2007 to 2013 there has been an increase in obesity, Type II DM and lack of physical activity in the community • This top down approach is not working
Precedent for no use of science • There is a precedent for not allowing the science of a subject be part of the recommendations. • For 10 years the sports medicine world discussed asthma. • It was only after many millions of euro had been spent on anti-doping protocols that the science was allowed to be used in diagnosis and management of asthma. • Experts should write the guidelines and non-experts may implement the guidelines
The prescription Part 3.
Pre-Participation Exam • History • Physical examination • Tests to include ECG, possibly others • What to tell the patient • Write the prescription in detail • Follow up
There are 12 key questions: RT Does the athlete have asthma (Wheezing), hay fever or coughing spells after exercise? CVS has anyone in the athlete’s family died suddenly before the age of 50 years Dizzy Has the athlete ever passed out during exercise or stopped exercising because of dizziness? CNS Does the athlete has a history of concussion GU Age of onset of menstruation and frequency.
There are 12 key questions: 7. Do you see a physician regularly for any particular problem 8. Meds: Does the athlete take any medication? 9. Allergies Is the athlete allergic to any medication or bee stings 10. Does the athlete have only one of any paired organ (eyes, ears, kidneys, testicles, and ovaries)? 11. Has the athlete ever broken a bone, had to wear a cast, or had an injury to any joint? 12. Does the athlete wish to discuss anything with the physician?
Physical examination • Emphasis on cardio-respiratory • Temp. BP, HR, RR at rest and with exercise, minutes of exercise per week • Weight, • Total body fat • Abdominal girth
The 90 second orthopedic screening exam Athletic Activity instruction Observation Stand facing examiner General habitus, AC joint Look at ceiling, floor, over both shoulders, Cervical spine motion Touch ears to shoulders Shrug shoulders Trapezius strength Abduct shoulders to Deltoid strength (Examiner resists at 90 degrees 90 degrees) Shoulder motion Full external rotation of arms Elbow motion Flex and extend elbows Arms at side, Elbows flexed at 90 degrees Pronate and supinate wrists
METS The energy cost of an activity can be measured in units called METS, which are multiples of your basal metabolic rate. One MET is the metabolic rate when one is sitting quietly in a normal temperature room. An increase in METs is based on speed and grade of thread mill (over estimate the oxygen capacity compared to oxygen consumption). The comparison of groups and the measure of exercise they are doing is important.
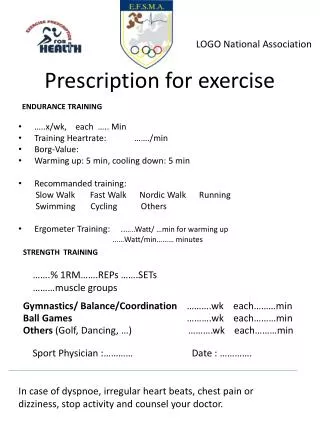
Original prescription FITT Minimal average top Frequency /week 3 5 6 Intensity light medium heavy sweating Type walk light jog heavy jog, run Time minutes 30 40 50
Tell the patient There are health-related benefits of regular physical activity that did not meet traditional criteria for improving fitness of exercise Exercise might also be considered as a fifth vital sign and should be recorded in patients' electronic medical records and routine histories, Simple things like walking instead of taking transit, and walking the dog make a big difference.
Tell the patient Patients ought to report how many minutes of physical activity they undertake in an average day and how many days a week such activity takes place. This measurement provides a score (in minutes per week) that can alert patients and clinicians to potential risks related to physical inactivity." People who took up playing football two or three times a week experienced reduced risk factors for cardiovascular disease, diabetes and the brittle-bone disease osteoporosis.
Modifiable Risk Factors • Hypertension • High fat saturated diet • Abnormalbloodlipidlevels (high total cholesterol, high levels of triglycerides, high levels of low-density lipoprotein or low levels of high-density lipoprotein (HDL) cholesterol). • Tobacco use (smoking or chewing tobacco, especially if started at a young age or in females). • Physical inactivity increases the risk of heart disease and stroke by 50% (reference).
Modifiable Risk Factors • Obesity is a major risk for cardiovascular disease and predisposes to diabetes 2. • Type 2 diabetes, which doubles the risk of coronary heart disease and stroke. • A chronically stressful life, social isolation, anxiety and depression increase the risk of heart disease and stroke. • One or two units of alcohol may lead to a 30% reduction in heart disease, but more than this level of alcohol consumption may damage the heart. • Medications may increase the risk of heart disease eg. contraceptive pill, hormone replacement therapy (HRT). • Left ventricular hypertrophy (LVH).
Non-Modifiable Risk Factors • Age, the risk of stroke doubles every decade after age 55. • Family’s history, cardiovascular disease indicates your risk. If a first-degree blood relative has had coronary heart disease or stroke before the age of 55 years (for a male relative) or 65 years (for a female relative) your risk increases. • Gender, males have a greater risk of heart disease than pre-menopausal woman. Once females reach the menopause, the risk of cardiovascular disease is similar. Men and women have the same risk of stroke.
Psychology is important • Identification • Pre-contemplation Phase • Contemplation Phase • Preparation Phase • Action Phase • Maintenance Phase • Motivation • Competence • Autonomy • Relatedness
Identification • Pre-contemplation Phase – the patient has not yet considered a lifestyle change. • Recommended action by the physician: educate the patient on the benefits to be achieved by initiating lifestyle changes. • Contemplation Phase – the patient thinks about commencing regular physical activity within the next 6 months recommended action by physician : as per Exercise Guidelines Document • Preparation Phase – the patient is ready to start exercising regularly within the next 30 days recommended action: as per Exercise Guidelines Document
Motivation • Competence • The feeling that they are sufficiently capable to affect a desired behavioural outcome. • This may be experienced as a self-belief in the ability to exercise and to feel comfortable in exercise settings. • Competence enhances the intrinsic motivation for the behaviour (i.e., being able to participate in physical activity).
Exercise prescription: Patients’ flow HD SEM Society / Healthcare system GP Physiotherapists Sport & Exercise Graduates Strength & C Personal trainers
The prescription contains • Warm up • Frequency • Intensity • Type • Time • Cool down • Stretch and agility • Strength and conditioning • Flexibility
Laboratory tests ECG and when a referral to a cardiologist is indicated (appendix 4.) Physiological assessment Physician supervised physiological exercise test is done with continuous monitoring of cardiac, pulmonary and metabolic parameters as needed. There is no simple set of guidelines for a physiological exercise test. The risk of CV events with exercise increase as a direct function of exercise intensity (vigorous > moderate > low exercise intensity) Clinically it is used to decide the cause of dyspnea and limitation to exercise. It is used to note ECG changes of exercise that may reflect ischemia, cardiac arrhythmia, exercise induced asthma, hypoxemia of exercise and other parameters
Clinical monitoring History Improved cardio-respiratory endurance Improved muscular endurance without symptoms Improved ability to do daily activities Physical examination BP, HR, RR at rest and with exercise, mins of exercise Weight, Reduced total body fat Reduced abdominal girth Blood tests Repeat CP ex test
The House of Lords, UK, Science and Technology Committee • The above group has launched a new short inquiry into sports and exercise science and medicine after the London Olympics. • Commenting, Lord Krebs, Chairman of the Committee, said: “There is an ever-growing body of evidence showing that increasing the amount of exercise people take can be of huge benefit in treating a wide range of chronic conditions. However, we are not convinced that health rofessionals currently have the skills or support to prescribe appropriate training regimes for their patients” (My, as President, emphasis).
SUMMARY of EPH • The science of exercise must not be dumbed down again • The patient must be central to all exercise endeavour and should include • PPE, • psychology, • exercise physiol principles being applied, • CPET as a clinical laboratory test available in clinical PFT laboritories and is our gold standard • follow up and reassessment is essential