Download
1 / 40
400 likes | 577 Views
Results of the 2002 Emergency Pediatric Services and Equipment Supplement (EPSES) to the National Hospital Medical Care Survey (NHAMCS). Division of Health Care Statistics Kimberly Middleton BSN MPH. Centers for Disease Control and Prevention National Center for Health Statistics. Overview.

E N D
Results of the 2002 Emergency Pediatric Services and Equipment Supplement (EPSES) to the National Hospital Medical Care Survey (NHAMCS) Division of Health Care Statistics Kimberly Middleton BSN MPH Centers for Disease Control and Prevention National Center for Health Statistics
Overview • Background • EPSES Methodology • Results • Next Steps
American Academy of Pediatrics Recommendations • A schedule of pediatricians on call to every ED • All EDs to establish transfer agreements with facilities with higher levels of pediatric care to ensure timely access to pediatric emergency care for critically ill and injured children
American Academy of Pediatrics Guidelines • All equipment and supplies listed, including age-appropriate and size-appropriate equipment for children of all ages and sizes from premature infants through adolescents • Each hospital must develop a method for storage and provide accessibility of medications and equipment for children
1998 NEISS Findings • Hospitals w/o pediatric dept, ward or trauma service usually transfer critically injured pediatric trauma patients • Nearly 10% of hospitals w/o pediatric intensive care unit (PICU) admit critically injured pediatric trauma patients • 7% of all hospitals admit pediatric patients requiring intensive care to adult intensive care unit (ICU) instead of transferring to hospital with PICU
1998 NEISS Findings cont’d • Few hospitals have protocols for obtaining peds consultation for peds emergencies • Appropriate sized equipment for infants and children was more likely to be missing than adult-sizes • A significant number of hospitals did not have adequate equipment to care for newborn emergencies.
Emergency Pediatric Services and Equipment Supplement (EPSES) • Funded by HRSA to replicate study of pediatric services done by NEISS in 1998. • Added as a supplement to the 2002-03 NHAMCS.
EPSES comparison • Findings: When compared to the NEISS study, the 2002 EPSES data did not show a difference in estimates. • Implication: There has been no increase in the availability of pediatric emergency services since 1998.
NHAMCS Methodology • National probability sample • Not Federal, military, or Veterans Administration facilities • Located in 50 states and D.C. • 4 stage sample design • 4 week reporting period • Data collected by Bureau of Census
EPSES Methodology • Short set of questions related to hospital services followed by a listing of 131 pieces of AAP recommended pediatric equipment. • Self-administered questionnaire
EPSES Response • Raw number of hospitals: 480 • # of hospitals with no ED: 83 (17%) • # of hospitals that refused: 51 (13%) • Number of participating hospitals: 346 • Response rate: 87%
EPSES concepts & measures • Pediatric Structure: • does not admit pediatric patients • admits pediatric patients, but has no separate pediatric ward • admits pediatric patients and has a separate pediatric ward.
EPSES concepts and measures • ED Pediatric Caseload: • Annual volume of ED cases by children under 18 • Percent of visits to an ED by children under 18 years of age • Availability of Pediatric Equipment • Totally supplied-100% of recommended equipment • Percent available out of all recommended supplies • Adequately supplied- above the median in terms of available pediatric equipment
Results • Structure • ED caseload • Services • Expertise • Equipment
Average Emergency DepartmentAnywhere, USA • Sees between 1500-7500 pediatric patients in a given year, which represents 20-30% of their ED caseload. • Hospital is not likely to have a pediatric ward. • Probably has a board certified emergency medicine attending, but unlikely to have a pediatric emergency medicine attending or pediatric attending. • Has about 80% of the recommended pediatric supplies and 5% are fully supplied.
Average Pediatric VisitAnywhere, USA • Average pediatric visit is to a hospital ED that has a large pediatric volume (>7500) • Hospital is more likely to have a separate pediatric ward and PICU (25%) • These EDs are more likely to have a board certified pediatric EM attending and a board certified pediatric attending when compared to the average hospital • Have 91% of recommended pediatric supplies and 20% of these EDs are fully supplied.
Among hospitals with 24hr EDs: • 10% do not admit pediatric patients • 52% admit pediatric patients but do not have a separate pediatric ward or department, i.e., one intended for exclusively treating children • 38% admit pediatric patients and have a separate pediatric ward or department
Distribution of EDs by the relative size of the pediatric ED patient mix and pediatric structure of the hospital: United States, 2002
Services for critically injured pediatric patients • 37% of all pediatric ED visits are for injury • 3% of EDs have a separate pediatric emergency service area (ESA) • 18% of hospitals with EDs,have a pediatric 23-hour observation unit • 16% of hospitals with EDs, have a coordinated pediatric trauma service • 10% of hospitals with EDs,have a PICU
Pyramid of pediatric ED cases 1.25% 5% 100%
Pediatric transfers • 53% of hospitals had written transfer agreements to facilities with a pediatric trauma service. • 57% of hospitals had written transfer agreements to facilities that have a pediatric intensive care unit.
Among EDs w/o critical care services, percent with written transfer agreements by inpatient pediatric structure, US 2002
Pediatric Transfers for Critically Injured Trauma Patients • Percent of hospitals w/o peds trauma service that transfer to another hospital • EPSES: 88%(NEISS 75% CI:41-100%) • Percent of hospitals w/o PICU that transfer to another hospital • EPSES: 89%(NEISS 91% CI:82-99%)
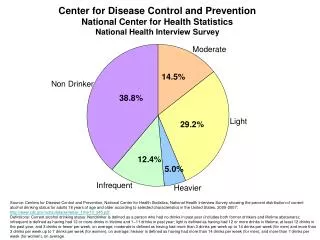
Attending Physician Specialty (available 24/7 in-house or on-call)
Availability of Pediatricians • Only 9% had a pediatrician on duty in the ED 24 hours/7days per week • On-call: 26% of hospitals had written protocols stating under what conditions a pediatrician would be called to the ED
Variation in availability of board certified attending physician specialty by inpatient pediatric structure
Totally Supplied • Only 10.8% of EDs answered YES to all 131 pediatric emergency supplies on the list. • Range: airway management (15.8%)- resuscitation medication chart, tape, or other dose estimation system (94.7%) • More supplies may be located in: NICU, OB, newborn nursery, central supply, pharmacy, nearby children’s or sister hospitals.
Distribution of the percent of pediatric supplies available in the ED: US 2002
Variation of supply availability score by inpatient pediatric structure, US 2002
What about hospitals that don’t admit and are undersupplied? • Of the 6% of hospitals in our sample that did not admit peds and were <85% supplied, all had other hospitals within the same county that either had peds beds or a separate peds ward. • Additional write in responses explained that some hospitals have EMS agreements to bypass their facility for nearby “sister” or children’s hospitals.
Next Steps • Currently combining 2002-03 data to provide in-depth analysis on ED pediatric care by combining EPSES variables (e.g. structure, expertise, equipment) with the NHAMCS visit file to look for relationships between items such as: • Medications prescribed • Diagnosis • Type of injury • Source of payment