Download
1 / 46
460 likes | 640 Views
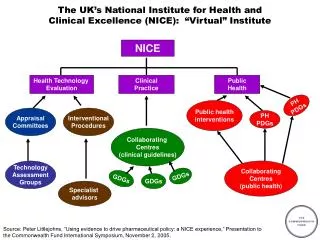
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Quality and Productivity Workshop 25 th September 2009. Quality and productivity: NICE’s experience to date. Peter Littlejohns Clinical and Public Health Director. NICE’s role.

E N D
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Quality and Productivity Workshop 25th September 2009
Quality and productivity: NICE’s experience to date Peter Littlejohns Clinical and Public Health Director
NICE’s role • Support best practice through encouraging the use of cost-effective interventions and discouraging the use of cost in-effective interventions • Views have been expressed that NICE should place more emphasis on the latter ( CMO report, Health Select Committee) • Two approaches : integrated or separate programme
2006 pilot to establish a designated programme • Criteria • Interventions are thought to be of equal or lesser effectiveness than a cheaper alternative • The annual resource cost to the NHS is in excess of £1 million • Recommendations on the use of the technology are not already covered by NICE guidance (published or in preparation) • Process • Development of scope and evidence base • Consultation • Scoping workshop • Outcomes • Many topics already covered • Many proposed topics not appropriate • 2 short clinical guidelines
“Disinvestment Programme” : lessons from the pilot • NICE already issuing disinvestment advice • over 200 in 2006 • Very few candidates for total disinvestment • antibiotics/ diagnostic tests ? • Lack of evidence • Often an issue of “values” rather than effectiveneness”
Current Approach • Topic selection and scoping • Cochrane Reviews • Optimal practice reviews (recommendation reminders -123 so far ) • Cost impact assessments • What else ?
Quality and ProductivityCentre for Health Technology Evaluation Carole Longson Director Centre for Health Technology Evaluation
Centre for Health Technology EvaluationGuidance Programmes • Interventional Procedures • Technology Appraisals • Evaluation Pathway for Medical Technologies • Diagnostic Technologies
Interventional Procedures Programme • Safety and efficacy programme Guidance on whether interventional procedures used for diagnosis or treatment are safe and efficacious enough for use
Technology Appraisal Programmes • How well does the drug work compared to standard practice in the NHS • How much does this course of action cost compared to standard practice in the NHS Difference in costs Difference in effects
More effective and less costly More effective and more costly Less effective and less costly Less effective and more costly The cost-effectiveness plane Cost + Technology Appraisals _ + Effect _
Technology Appraisals - the results 342 individual recommendations in 166 technology appraisals
The Evaluation Pathway for Medical Technologies • New Advisory Body - MTAC • Process and methods being designed with a quality and productivity focus • Characteristics of the products likely to be selected for routing through the pathway • demonstrable therapeutic gain and • the ability to drive significant efficiencies
More effective and less costly More effective and more costly Less effective and less costly Less effective and more costly The cost-effectiveness plane Cost + _ + Effectiveness _ MTAC
Technology Evaluation - optimising resources • There is a tension in encouraging uptake of more effective but more costly technologies and the present economic climate in the NHS • Optimising resources lies at the heart of our technology evaluation methodology • Can NICE technology evaluation programmes enhance their support for a ‘quality and productivity’ focus? • Greater emphasis on technologies that have the potential to improve clinical quality with reduced overall resource use
Centre for Clinical PracticeClinical Guidelines Christine Carson Programme Director, Centre for Clinical Practice
Clinical Guidelines • The standard and short guideline programme • Broad guidance covering aspects of assessment, diagnosis, referral, treatment, management and care of a particular condition • Recommendations are based on evidence of effectiveness and cost effectiveness to improve the quality of care offered at the right time, resulting in long-term savings • Incorporate or update technology appraisals (TAs) Interventional Procedures & public guidance when relevant • Includes new and existing interventions
Opportunities within guidelines • Current methodologies and processes frequently lead to explicit recommendations to discontinue many existing practices and interventions. • For example, the prostate cancer CG, of 105 recommendations, just under a quarter (25) were recommendations ‘not recommending’ interventions or first line treatments ‘Positron emission tomography (PET) imaging for prostate cancer is not recommended in routine clinical practice’
Disinvesting in ineffective practice Evidence of ineffectiveness results in recommendations in CG changing long standing clinical practices, for example: ‘Antibiotic prophylaxis against infective endocarditis is not recommended for people undergoing dental procedures, non-dental procedures… upper and lower gastrointestinal tract… gynaecological and obstetric procedures, and childbirth.’ OR ’A no antibiotic prescribing strategy or a delayed antibiotic strategy should be agreed for patients with: Acute otitis media, acute sore throat, common cold etc…’
Switching to more effective practice (1) • Recommendations are developed for interventions to be used in preference to another because they are cost effective, for example, in the ADHD CG ‘…for adults with ADHD stabilised on medication but with persisting functional impairment, or where there has been no response to drug treatment, a course of either group or individual CBT… should be considered. Group therapy is recommended as the firstline psychological treatment because it is the most cost effective.’
Switching to more effective practice (2) OR Recommendations in CG suggest when to use specific interventions, for example, the CKD CG recommends: • ‘when testing for the presence of haematuria, use reagent strips rather than urine microscopy. • Evaluate further if there is a result of 1+ or more. • Do not use urine microscopy to confirm a positive result
Optimising interventions Recommendations also include intervention thresholds, specifically early identification and who to treat, for example, Lipid Modification CG. • ‘for the primary prevention of CVD in PC, a systematic strategy should be used to identify people aged between 40 and 74 who are likely to be at high risk. • People should be prioritised on the basis of an estimate of their CVD risk before a full formal risk assessment…’ • Costings estimated additional costs of £13.4 million for systematic CVD risk assessment • Better identification of those at high risk CVD is expected to lead to reduction in CVD events 13,500 per annum saving £46.5 million per year.
Clinical guidelines: optimising resources • Substantial and continuing contribution to helping the NHS use resources effectively • We could do more by, for example, doing more ‘service guidance’ alongside clinical recommendations • Should we consider providing ‘resource-neutral’ guidance? But what would be the consequences for service quality – and the credibility of our guidance with NHS professionals?
NICE, Public Health and Prevention Professor Mike Kelly Director of the Centre for Public Health Excellence
Key topics in published and planned public health guidance • Physical activity • Smoking and tobacco • Sexual health • Alcohol • Drugs • Maternal and child health • Health and work • Older people’s health and wellbeing • Cancer • Immunisation • Accidental injury. • Obesity • Mental well being • Cardio vascular disease. • Diabetes • Communicable disease
Some QALY Values Preventing uptake of smoking by children and young people £49-£1,690 Identifying people at risk £1,399-£5,992 £2,979-£4,692 Management of long term sickness and incapacity for work cost saving • Smoking cessation £292 - £1677 • Physical activity £20 - £427 • Substance misuse cost saving • Workplace smoking cessation cost saving
Calculating the Cost Impact • Production costs in NICE • Costs to the service of implementation • Direct costs • Current practice • Displacement / opportunity costs • Savings • Degree of implementation • Benefits • Immediate • Medium term • Long term
Implications for the health gradient Hi Health state Lo Lo Hi Social difference
How public health guidance can release resources in the medium/long term • Prevention is cost effective and can be cost saving. • Reductions in the disease burden. • Development of efficiencies in systems and organisation. • Getting effective technologies to where they will have the greatest benefit. • Helping to build the local building business case.
The implementation perspective Jennifer Field, Associate Director, Implementation
Forward planner • Using the forward planner • The forward planner helps people plan for and implement NICE guidance by: • summarising published guidance organisations may still be implementing • listing forthcoming guidance to help NHS bodies plan ahead • The forward planner is an Excel spreadsheet. The data can be sorted by any column. ‘Auto filter' has been added to the file so that types of data can be selected, such as published guidance, or technology appraisals. http://www.nice.org.uk/page.aspx?o=298522
The commissioning guides • Topic specific and web-based • Provide or signpost information on key clinical and service-related issues for commissioners to consider – underpinned by the relevant guidance. • Contain a commissioning tool - interactive resource to help estimate and inform the level of service needed locally, as well as the cost of local commissioning decisions. Registration required
NICE quality standards • A set of specific, concise statements acting as markers of high quality, cost effective care across a pathway or a clinical area. • Accompanied by measures • NICE quality standards are derived from the best available evidence.
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Quality and Productivity Workshop 25th September 2009