Download
1 / 23
260 likes | 570 Views
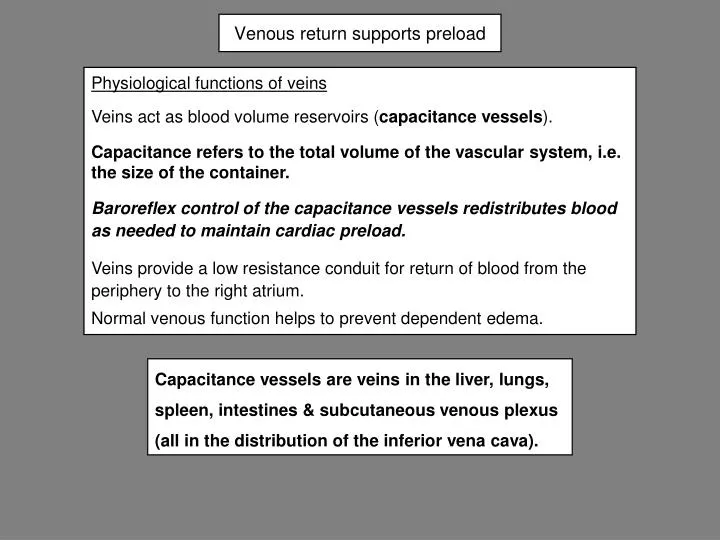
Venous return supports preload. Physiological functions of veins Veins act as blood volume reservoirs ( capacitance vessels ). Capacitance refers to the total volume of the vascular system, i.e. the size of the container.

E N D
Venous return supports preload Physiological functions of veins Veins act as blood volume reservoirs (capacitance vessels). Capacitance refers to the total volume of the vascular system, i.e. the size of the container. Baroreflex control of the capacitance vessels redistributes blood as needed to maintain cardiac preload. Veins provide a low resistance conduit for return of blood from the periphery to the right atrium. Normal venous function helps to prevent dependent edema. Capacitance vessels are veins in the liver, lungs, spleen, intestines & subcutaneous venous plexus (all in the distribution of the inferior vena cava).
67% of the blood volume is present on the venous side of the circulation • At rest 2/3 of the blood volume is present on the venous side of the circulation because the veins are the most compliant part of the circulation. • Venous compliance is ~ 20 times greater than arterial compliance. • The veins are called capacitance vessels because their large compliance allows veins to store blood at low pressure.
15 to 25 mm Hg 2 15 mmHg 2 to 7 mm Hg Venules & small peripheral veins Head & neck veins Large peripheral veins Thoracic veins abdominal veins Rt atrium 22 % of blood volume 45% of blood volume Pressures at rest, recumbent, in the systemic veins In recumbency the pressures in the head and neck veins are similar to those in the periphery below the heart 22 + 45 = 67% of blood volume is contained in the systemic veins
~ zero mm Hg in superficial neck veins Head & neck veins -10 mm Hg in sagittal sinus In the upright position veins in the leg constrict to minimize venous volume & shift blood toward the heart Rt atrium ~ zero mm Hg 300 to 800 ml of blood pools in the legs on standing abdominal veins There is a continuous pressure gradient from heart to foot due to the effect of gravity Thoracic veins Large peripheral veins Venules & small peripheral veins 100 to 125 mm Hg at the foot Pressures in the systemic veins in the upright position
CVP & right atrial pressure • Central venous pressure • CVP represents preload for the right atrium • CVP is determined by blood volume and venous capacitance • CVP is very close to right atrial pressure • Normal right atrial pressure is +2 to +7 mm Hg in recumbency • Range of right atrial pressures: • Minimum -3 to - 5 mm Hg at very high cardiac output or after severe hemorrhage • Maximum 20 to 30 mm Hg in severe heart failure
h Level of Rt. atrium Estimating CVP in the upright position In the dependent position the veins on the back of the hand are engorged due to the height (h) of the column of blood from the right atrium to the hand As the hand is raised, the height of the column decreases. When the hand is raised above the level of the right atrium (dotted line) the veins collapse. The height of the hand above the atrium (4th intercostal space) at the point of collapse equals the right atrial pressure.
Flow, pressure and resistance in the venous system • In the venous system, venous return (VR, blood flow at the entrance to the right atrium) is affected by • Changes in venous capacitance • Changes in vascular resistance • Capacitance is more important in the venous system than resistance. • DP is the pressure gradient from the left ventricle to to the right atrium • Rvis the resistance to venous return • Rvis affected by sympathetic tone and by mechanical impingement on the veins.
Sympathetic tone regulates venous capacitance and resistance • Stimulation of sympathetic nerves to veins causes • Constriction (decreased capacitance) • Increased venous resistance Rv • Sympathetically mediated venoconstriction • helps maintain venous return in the standing position • maintains venous return and preload during exercise • is part of the baroreflex response to hypotension or hypovolemia Baroreflex mediated constriction acts mostly on the smaller veins & venules to decrease capacitance & therefore shift blood toward the heart constriction
As the veins constrict, the heart tends to expand ↑ sympathetic nerve activity • ↓ capacitance (peripheral veins) A decrease in sympathetic nerve activity will have the opposite effect. Blood shifts to heart ↑ end diastolic volume ↑ stroke volume ↑ cardiac output A decrease in venous capacitance (diameter) also increases venous resistance which should decrease flow to the heart. However, venous resistance is only a small part of total peripheral resistance, so this effect is negligible. TPR is mainly determined by arteriolar resistance.
Large veins • Resistance is near zero when wide open • Veins are compressed at their entry to the thorax • Superficial neck veins are partly collapsed • Arm veins angle over 1st rib • Abdominal veins are partly collapsed due to pressure from viscera • Compression of the large veins increases resistance resulting in peripheral venous pressures of 4 to 7 mm Hg • Increasing right atrial pressure above 4 to 7 mm Hg causes distention of large veins. • Further increases in RAP increase peripheral venous pressure. Mechanical resistance to flow in large veins
Intra-abdominal pressure & venous resistance • Normal recumbent intra-abdominal pressure is ~ 6 mm Hg. • Intra-abdominal pressure may increase up to 15 to 30 mm Hg with: • Advanced pregnancy • Large intra-abdominal tumors • Ascites (intra-peritoneal edema fluid) • Severe obesity • Venous pressure must equal or exceed intra-abdominal pressure for flow to occur
↓ Arterial pressure Baroreceptors Vasomotor center ↑ Sympathetic activity + Constrict capacitance vessels ↑ venous return ↑ Preload ↑ Stroke volume ↑ CO Splanchnic circulation & baroreflex Baroreflex response to hypotension also includes effects on arterioles and heart The baroreflex does not affect veins feeding the superior vena cava.
artery vein In a closed system like the circulation, gravity does not affect flow Recumbent, circulation below heart P1 = 100 mm Hg P1 - P2 = 100 - 0 P2 = Zero mm Hg Standing Hydrostatic pressure due to gravity Pg = rgh; or Pg ~ h r = density g = acceleration of gravity h = height of column 100 mm Hg Zero mm Hg Pressure difference driving flow Arterial side: 100 + Pg Venous side: zero minus Pg DP = 100 + Pg - Pg = 100 mm Hg Gravitational effects on arterial & venous side cancel h
Standing, pressure gradient above heart Pg ~ h h 100 mm Hg Zero mm Hg Gravitational effect on the circulation in the upper body Pressure difference driving flow Arterial side: 100 - Pg mm Hg Venous side: Pg mm Hg DP = 100 - Pg + Pg = 100 mm Hg Gravitational effects on arterial & venous side cancel They are equal in magnitude but opposite in direction
25 mm Hg is capillary hydrostatic pressure Recumbent P1 = 100 mm Hg Standing, body below heart 25 mm Hg P1 - P2 = 100 - 0 P2 = Zero mm Hg 100 mm Hg Zero mm Hg In the standing position Pg causes increased venous pressure in the dependent areas. The veins have a large compliance so the increased pressure increases the volume of blood in the dependent venules & veins (“venous pooling”). Increased pressure increases capillary pressure and filtration. h Venous pooling 300 to 800 ml of blood may pool in dependent areas Venous pressure in foot may reach 90 to 100 mm Hg when standing still. Pooled blood is not stagnant; flow continues. (25 + Pg) mm Hg Effect of gravity in a compliant system: dependent pooling of blood
Effect of gravity in a compliant system:Negative venous pressure in the head In the standing position Pg is negative above the heart (the weight of the blood causes it to distribute toward the thorax). Pressure in deep veins above the heart may become negative (sub-atmospheric). Pressure in the sagittal sinus is - 10 mm Hg In superficial veins in the head & neck pressure decreases to zero as blood “falls” to the heart so these veins intermittently collapse and open. They collapse when venous pressure = zero; collapse causes upstream pressure to increase & the veins open. Deeper veins remain open because they are tethered by surrounding tissues. Standing, head above heart (25 - Pg) mm Hg h 100 mm Hg Zero mm Hg
Pc p i Pi Edema in dependent areas is limited by protective mechanisms. • In legs & feet interstitial pressure & volume increase when standing, some swelling may occur, but significant edema does not occur normally. • Protective mechanisms against edema formation: • Autoregulation:Initial shift of blood to legs stretches arterioles, autoregulation (myogenic constriction) limits the increase in capillary hydrostatic pressure • Balance of Starling forces: Capillary hydrostatic pressure filtration plasma oncotic pressure, interstitial oncotic pressure, interstitial hydrostatic pressure • Lymph flow removes filtrate from the interstitial space: • interstitial hydrostatic pressure fluid & protein uptake by lymph vessels • lymph vessel contractions lymph flow, removes filtrate
100 80 60 40 20 Muscle pump & venous valves Post thrombotic limb Muscle “pump” Normal Venous pressure in foot, mm Hg Standing Standing Walking 10 20 30 40 Standing still Walking Seconds When standing still venous pressure in the foot approaches 90 mm Hg. Normally during walking the muscular pump assists venous return so the volume of blood in the leg veins and venous pressure are lowered.
140 obstructed 120 post thrombotic Venous pressure, mm Hg 100 varicose 80 normal 60 walking Standing Standing 40 20 Seconds 0 30 60 90 Effect of venous disease on venous pressure in foot Venous pressure is elevated in chronic venous disease. Damage to the valves or a deep venous thrombosis impairs the muscle pump. Pressure in cutaneous veins remains elevated even during exercise. Prolonged elevated pressure leads to an inflammatory reaction, ulceration & other pathological changes in the skin.
Respiratory movements affect venous return by changing the pressure outside the vena cava with each breath Inspiration: Thorax expands Pressure outside thoracic vena cava decreases, vessel dilates. Diaphragm descends, abdominal organs compress abdominal vena cava Blood pumped toward heart Expiration: Thorax relaxes Pressure outside thoracic vena cava increases, vessel compressed. Diaphragm ascends, abdominal pressure decreases, abdominal vena cava expands Vena cava fills from lower body
respiration blood volume Sympathetic tone limb muscle contractions Peripheral venous pressure Venous pressure gradient venous return end diastolic ventricular volume stroke volume cardiac output Factors assisting venous return When cardiac output increases, increases in sympathetic stimulation of veins, respiration and muscle activity act rapidly to increase venous return. Blood volume may also increase with increased fluid intake and decreased excretion of urine.
a c v Venous pressure waves in cardiac cycle a wave: right atrial contraction c wave: upslope due to bulging of tricuspid (or mitral) valve into atrium; pressure drops when ventricle ejects blood v wave: atrial pressure increases during ventricular ejection as atrium fills; pressure drops when tricuspid valve opens Venous pressure may be estimated as the height of blood in the external jugular vein with the vein occluded distally. This pressure is an estimate of preload for the right ventricle. Elevated pressure suggests ventricular dysfunction.
Because the vascular system is a closed circuit, failure of the left ventricle leads to failure of the right ventricle Left ventricular failure Early diagnostic signs of heart failure include breathlessness on exercise, limitations of physical activity, orthopnea, pulmonary rales, peripheral edema, and raised jugular venous pressure. (Vascular Health and Risk Management, vol 7, p 591 2011) CO Left atrial pressure Pulmonary venous, capillary pressure Pulmonary capillary pressure Pulmonary edema Pulmonary artery pressure dyspnea afterload to Rt. ventricle Rt. Ventricular failure Systemic venous pressure Dependent edema