Download
1 / 40
420 likes | 589 Views
Health effects of radiation exposure. Tilman A Ruff Nossal Institute for Global Health, University of Melbourne Advisor: Australian Red Cross, AusAID/UNICEF Consultant: GSK Biologicals, Novartis Vaccines Medical Association for Prevention of War

E N D
Health effects of radiation exposure Tilman A Ruff Nossal Institute for Global Health, University of Melbourne Advisor: Australian Red Cross, AusAID/UNICEF Consultant: GSK Biologicals, Novartis Vaccines Medical Association for Prevention of War International Campaign to Abolish Nuclear Weapons Hunter’s Hill Inquiry, Sydney 4 July 2008
Overview • Overview of radiation • Sources of environmental radiation • Health effects of radiation
Radiation Basics Radiation – Energy in transit: • electromagnetic waves (gamma-γ or x-ray), or • high speed particles ( alpha-α, beta-β, neutron-η, etc.) Ionizing Radiation – Radiation with sufficient energy to remove electrons during interaction with an atom, causing it to become charged or ionized • Can be produced by spontaneous radioactive decay or by accelerating charged particles across an electric potential (eg x-rays)
Introduction • What is ‘radiation’? • Electromagnetic energy • Spectrum
Ionizing vs Non-ionizing • Ionizing radiation has high energy and displaces electrons from their orbits creating charged atoms (ions)/molecules • Creates DNA damage • Outright cell death • Bystander effect • Genomic instability • Non-ionizing radiation creates heat due to low energy eg infrared, MRI
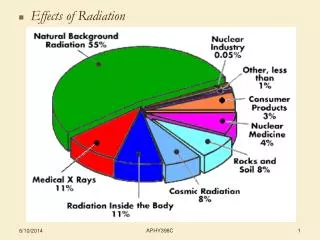
Ionizing Radiation Sources • Average global dose: 2.4 mSv
Multiple exposure pathways • External - often gamma • Most easily measured • Direct contact – skin • Internal • Inhale – gas, dust, aerosol • Ingest • Food – many radioisotopes bioconcentrated • Water • Environmental source esp young children • Wounds
Radiation Basics Radioactivity – 1 Becquerel (Bq)= 1 radioactive disintegration per sec Absrbed dose – 1 Gray (Gy) = 1 joule of energy deposited per kilogram Equivalent dose (biological effect) – Sievert (Sv) the unit of absorbed dose equivalent. The energy absorbed by the body based on the damaging effect for the type of radiation. Sv =Gray x Quality Factor
Radiation Quantities and Units • Biological equivalent dose: Sievert (Sv) = joules per kilogram • Relates to the amount of radiation harm in biological tissues • Beta, gamma, and x-ray Sv = Gy • Particle weightings (electrons = 1; neutrons = 5; alpha = 20) • Biological effective dose: Sievert (Sv) = equivalent dose weighted for susceptibility to harm of different tissues
Radon • Produced from radium in decay chain of uranium • Escapes into air – short lived decay products emit alpha particles – stick to dust, inhaled, deposit in lung – high but localised radiation • Second most important cause lung cancer
Radon • Average outdoor levels: 5-15 Bq/m3 • Global indoor average: 39 Bq/m3 • Action levels – generally 200-400 Bq/m3 (Australia 200) • Risk of lung cancer increases by 16% per 100 Bq/m3 increase in radon • Relationship linear with no threshold • Risk synergistic with smoking • Some (weak) evidence of increased effect at low dose rate
Radon risk per 1000 of lung cancer by age 75 y WHO Factsheet 291 June 2005
Cell Sensitivity • Cells most affected: • Rapidly dividing cells: • small intestines, bone marrow, hair, fetus
Ionising radiation • Capacity to damage core genetic blueprint - DNA → cancer → other health effects → genetic damage • Lethal dose can have equivalent energy to heat in a cup of coffee • Many different isotopes • Behave differently biologically
Biological Effects of Radiaton • Deterministic effects (>100mSv) • Threshold • Increased dose = increased damage • Stochastic (probabilistic) effects (no safe threshold) • Increased dose = increased probability of damage but not severity
Delayed Somatic Effects • 1. Cancer: solid tumors • Increased risk • Latency period: 10+ y • 2. Cancer: leukemia • Increased risk • Latency period: 5+ y • 3. Degenerative effects (LSS, not sure at low doses) • Life shortening (not sure) • Heart disease, stroke; digestive, respiratory, hemopoietic systems
Cancer Risks • Normal cancer risk (Australia): • About 1:2 men get cancer by age 85 • About 1:3 women get cancer by age 85 • Normal mortality: • 29% of Australians die primarily from cancer • 49.3 % die primarily or as a consequence of cancer Cancer in Australia: an overview 2006, AIHW
Cancer Risks • Linear, no threshold • Increased risk of cancer from 1 mSv of radiation: • Solid tumor cancer risk about 1 in 10,000 • Leukemia risk about 1 in 100,000 • Increased risk of cancer mortality about half those : • Solid cancer deaths: about 1 in 20,000 • BEIR VII 2005
Cancer risks vary • Infancy 3-4x increased risk cf 20-50y • Female infants 2x risk of male infants • Female risk of cancer is 37.5% greater than males • 50% greater risk of solid tumours • Less risk leukaemia • BEIR VII 2005
Fetal radiation risk • There are radiation-related risksthroughout pregnancy that are related to the stage of pregnancy and absorbed dose • Radiation risks are most significant during organogenesis and in the early fetal period, somewhat less in 2nd trimester, and least in 3rd trimester Most risk Less Least
Leukaemia and cancer • The relative risk may be as high as 1.4 (40% increase over normal incidence) due to a fetal dose of 10 mSv • For an individual exposed in utero to 10 mSv, the absolute risk of cancer at ages 0-15 is about 1 excess cancer death per 1,700
Nuclear industry workers 1 • 15 country retrospective cohort study of cancer mortality auspiced by IARC • Largest such study ever conducted • Workers involved in fuel enrichment or reprocessing, reactors, weapons or isotope production (excl uranium mining) • 407,391 workers (90% male): • employed ≥ 1 y • monitored for external photon (X and gamma) radiation • > 90% whole body dose from external photons rather than neutrons or internal exposures • Total FU 5.2 million person y
Nuclear industry workers 2 • Doses to colon used for all and solid cancer, active bone marrow for leukemia analyses, lagged by 2 y for leukemia and 10 y for other cancers • Doses: • Average 19.4 mSv • 90% < 50 mSv • < 0.1% > 500 mSv • Total deaths 6516 from cancer other than leukemia, 196 from leukemia excl CLL
Nuclear industry workers 4 • Mortality from all cancers except leukemia – central estimate 2-3 times higher than linear extrapolation from atomic bomb survivors • Current recommended 5 y occup dose limit of 100 mSv → 9.7% (1.4 - 19.7%) increase in cancer excl leukemia • For leukemia excl CLL 100mSv → 19% (<0 - 84.7%) increase Cardis E, et al. BMJ 2005 (29 June 2005) BMJ,doi:10.1136/bmj.38499.599861.EO
‘Routine’ radiation releases • First large meta-analysis of data on childhood leukaemia and nuclear facilities • International peer-reviewed journal • Multiple sites, different populations, different time periods, collected differently are difficult; findings more likely to be significant • No major sources of bias identified • Countries with poorer environmental standards eg Russia, China and developing countries are excluded, so likely best case scenario • Effects robust to different types of analyses
‘Routine’ radiation releases • Point estimates are all above 1 • A number of important findings are statistically significant eg all of the results for childhood leukaemia incidence • Association of young age and closeness to a nuclear facility with higher risk are biologically plausible, suggest dose-response effect • Heightened sensitivity of children to radiation, and leukaemia as most radiation sensitive cancer with shortest latent period support biological plausibility • funded by the US DOE
German Childhood Cancer Registry data 1980 – 2003, <5y • Matched case-control study • 593 leukemia cases • Odds ratio for leukemia 2.19 (lower 95% CI 1.51) for residence within 5 km of nuclear power plant
1592 cases, 4735 controls • Odds ratio 1.47 (lower 95% CI 1.16) for inner 5 km zone