Download
1 / 1
10 likes | 140 Views
Do all colorectal polyps require pathological examination?. Polyps’ size. ≤ 5 mm. 6 – 9 mm. ≥ 10 mm. all. Number n (%). 2038 (51.3). 589 (14.8). 1343 (33.8). 4360. Adenomatous polyps n (%). 1361 (66.8). 483 (82.0). 1290 (96.1). 3134 (71.9). Advanced adenoma n (%). 280 (13.7).

E N D
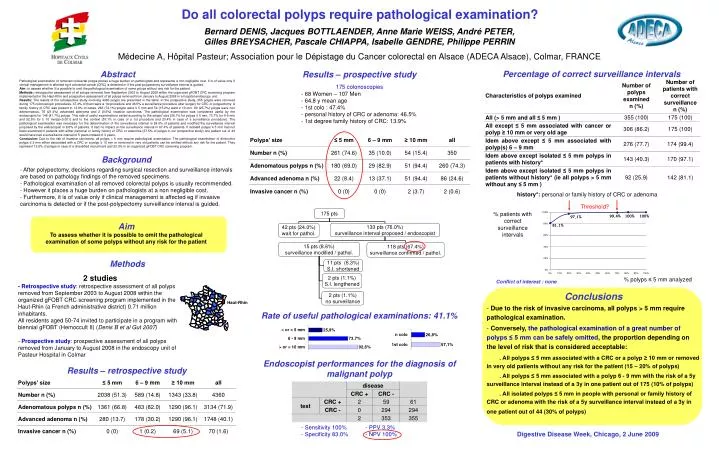
Do all colorectal polyps require pathological examination? Polyps’ size ≤ 5 mm 6 – 9 mm ≥ 10 mm all Number n (%) 2038 (51.3) 589 (14.8) 1343 (33.8) 4360 Adenomatous polyps n (%) 1361 (66.8) 483 (82.0) 1290 (96.1) 3134 (71.9) Advanced adenoma n (%) 280 (13.7) 178 (30.2) 1290 (96.1) 1748 (40.1) Invasive cancer n (%) 0 (0) 1 (0.2) 69 (5.1) 70 (1.6) Bernard DENIS, Jacques BOTTLAENDER, Anne Marie WEISS, André PETER, Gilles BREYSACHER, Pascale CHIAPPA, Isabelle GENDRE, Philippe PERRIN Médecine A, Hôpital Pasteur; Association pour le Dépistage du Cancer colorectal en Alsace (ADECA Alsace), Colmar, FRANCE Percentage of correct surveillance intervals Abstract Results – prospective study Pathological examination of removed colorectal polyps places a huge burden on pathologists and represents a non negligible cost. It is of value only if clinical management is affected eg if colorectal cancer (CRC) is detected or if the post-polypectomy surveillance interval is guided. Aim: to assess whether it is possible to omit the pathological examination of some polyps without any risk for the patient. Methods: retrospective assessment of all polyps removed from September 2003 to August 2008 within the organized gFOBT CRC screening program implemented in the Haut-Rhin and prospective assessment of all polyps removed from January to August 2008 in a hospital endoscopy unit. Results: The results of the retrospective study involving 4360 polyps are presented in the table. In the prospective study, 355 polyps were removed during 175 colonoscopic procedures. 47.4% of them were a 1st procedure and 46.5% a surveillance procedure after surgery for CRC or polypectomy. A family history of CRC was present in 13.9% of cases. 263 (74.1%) polyps were ≤ 5 mm and 54 (15.2%) were ≥ 10 mm. 90 (25.7%) polyps were non adenomatous, 76 (21.4%) advanced adenoma and 2 (0.6%) invasive carcinoma. The pathological examination was considered useful by the endoscopist for 148 (41.7%) polyps. This rate of useful examinations varied according to the polyps’ size (26.1% for polyps ≤ 5 mm, 73.7% for 6-9 mm and 92.5% for ≥ 10 mm)(p<0.001) and to the context (57.1% in case of a 1st procedure and 23.4% in case of a surveillance procedure). The pathological examination was necessary for the determination of the surveillance interval in 24.0% of patients and modified the surveillance interval proposed by the endoscopist in 8.6% of patients. It had no impact on the surveillance interval in 67.4% of patients. If isolated polyps ≤ 5 mm had not been examined in patients with either personal or family history of CRC or adenoma (37.5% of polyps in our prospective study) one patient out of 44 would have had a surveillance interval of 5 years instead of 3 years. Conclusion: Due to the risk of invasive carcinoma, all polyps > 5 mm require pathological examination. The pathological examination of diminutive polyps ≤ 5 mm either associated with a CRC or a polyp ≥ 10 mm or removed in very old patients can be omitted without any risk for the patient. They represent 13.8% of polyps in case of a diversified recruitment and 22.3% in an organized gFOBT CRC screening program. • 175 colonoscopies • 68 Women – 107 Men • 64.8 y mean age • 1st colo : 47.4% • personal history of CRC or adenoma: 46.5% • 1st degree family history of CRC: 13.9% Background • After polypectomy, decisions regarding surgical resection and surveillance intervals are based on pathology findings of the removed specimens. • - Pathological examination of all removed colorectal polyps is usually recommended. • However it places a huge burden on pathologists at a non negligible cost. • - Furthermore, it is of value only if clinical management is affected eg if invasive carcinoma is detected or if the post-polypectomy surveillance interval is guided. history*: personal or family history of CRC or adenoma Threshold? % patients with correct surveillance intervals Aim To assess whether it is possible to omit the pathological examination of some polyps without any risk for the patient Methods 2 studies - Retrospective study: retrospective assessment of all polyps removed from September 2003 to August 2008 within the organized gFOBT CRC screening program implemented in the Haut-Rhin (a French administrative district) 0.71 million inhabitants. All residents aged 50-74 invited to participate in a program with biennial gFOBT (Hemoccult II) (Denis B et al Gut 2007) - Prospective study: prospective assessment of all polyps removed from January to August 2008 in the endoscopy unit of Pasteur Hospital in Colmar % polyps ≤ 5 mm analyzed Conflict of interest : none • Conclusions • Due to the risk of invasive carcinoma, all polyps > 5 mm require pathological examination. • Conversely, the pathological examination of a great number of polyps ≤ 5 mm can be safely omitted, the proportion depending on the level of risk that is considered acceptable: • . All polyps ≤ 5 mm associated with a CRC or a polyp ≥ 10 mm or removed in very old patients without any risk for the patient (15 – 20% of polyps) • . All polyps ≤ 5 mm associated with a polyp 6 - 9 mm with the risk of a 5y surveillance interval instead of a 3y in one patient out of 175 (10% of polyps) • . All isolated polyps ≤ 5 mm in people with personal or family history of CRC or adenoma with the risk of a 5y surveillance interval instead of a 3y in one patient out of 44 (30% of polyps) Haut-Rhin Rate of useful pathological examinations: 41.1% Endoscopist performances for the diagnosis of malignant polyp Results – retrospective study • Sensitivity 100% - PPV 3.3% • Specificity 83.0% - NPV 100% Digestive Disease Week, Chicago, 2 June 2009