Download

1 / 18
180 likes | 321 Views
Policy-Relevant Determinants for the Control of Macrolide-Resistant Streptococcus pneumoniae : Do International Comparisons Help?. Harbarth S, Monnet DL, Pechère JC, Cars O. BACKGROUND. Evaluating policy-relevant determinants of antibiotic overuse and bacterial resistance is a complex task.

E N D
Policy-Relevant Determinants for the Control of Macrolide-Resistant Streptococcus pneumoniae: Do International Comparisons Help? Harbarth S, Monnet DL, Pechère JC, Cars O.
BACKGROUND • Evaluating policy-relevant determinants of antibiotic overuse and bacterial resistance is a complex task. • Standardized assessment of these determinants may enable cross-cultural comparisons and allow policy makers to identify and implement those control measures that are the most likely to be successful.
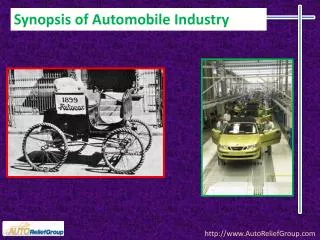
Penicillin-resistant pneumococci and outpatient AB-use 60 Taiwan 50 Spain France 40 USA Greece 30 Portugal Penicillin-nonsusceptible S. pneumoniae (%) This is where a large graphic or chart can go. Ireland 20 Canada Luxemburg Iceland Italy Austria Belgium UK 10 Australia Germany Albrich, Monnet & Harbarth, Emerg Infect Dis 2004 Finland Sweden Denmark Netherlands Norway 0 0 10 20 30 40 Total antibiotic use (DDD/1000 pop/day)
OBJECTIVES • The purpose of this retrospective, ecologic study was to explore macro-level determinants explaining the large variation in MRSP prevalence in 14 European countries. • Specifically, we attempted to test different hypotheses (e.g., antibiotic usage patterns, population characteristics) linked to low or high MRSP prevalence.
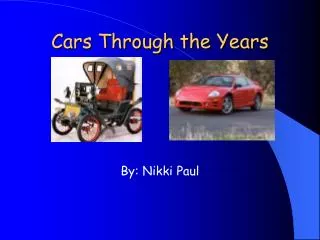
Prescriberfactors Patient factors Antibiotic overuse and misuse Antibiotic-resistant pneumococci Cultural influences Social determinants Regulatory practices Macro-level determinants influencing AB overuse Harbarth et al, Emerg Infect Dis 2002; 8: 1460-1467
METHODS • An extensive list of all possible determinants that might explain variations in MRSP prevalence was established. • Data on MRSP prevalence and explanatory factors were retrieved from electronic databases, reports from multinational and national surveillance systems, and international organizations. • Correlations were assessed with the 2-tailed Spearman coefficient for non-parametric correlations.
Lower use of macrolides • (less exposed, shorter duration) • Lower use of other antimicrobials • Better compliance (dose, intervals) • Pre-school facilities • Long-term care? • Better living conditions • Socio-economic status • Climate? • Less travel • Different clones More rational use of antibiotics? Lower Proportion of Macrolide-R S. pneumoniae in Community-Acquired RTIs Less cross-transmission? Better protection against disease? Different population? • Age (extremes) • Respiratory and other diseases • Vaccination • Breast feeding
Macrolide-Resistant Streptococcus pneumoniae and Macrolide Consumption in EU Member States, 1997-1998 Sources: Alexander Project, FINRES, STRAMA, DANMAP, and Cars O, et al. Lancet 2001; 357: 1851-3.
Macrolide-R S. pneumoniae(%) and Antimicrobial Consumption in Europe This is where a large graphic or chart can go. Source for resistance data: Alexander Project. Source for antimicrobial consumption data: Cars O, et al. Lancet 2001; 357: 1851-3.
Macrolide-R S. pneumoniae(%): Factors Affecting Compliance with Antibiotic Treatment This is where a large graphic or chart can go. Source: EUROBAROMETER 2002.
Macrolide-R S. pneumoniae(%): Factors That Might Facilitate Cross-Transmission This is where a large graphic or chart can go. Sources: Danish National Institute of Social Research, EC Eurostat, and European Travel Commission (ETC) Tourism Statistics.
Macrolide-R S. pneumoniae (%): Population Characteristics and Protection against Disease This is where a large graphic or chart can go. Sources: U.S. Bureau of the Census, EC Eurostat, WHO Regional Office for Europe, and Fedson DS. Clin Infect Dis 1998;26:1117-23.
Macrolide-R S. pneumoniae(%):Economic and Health Care System This is where a large graphic or chart can go. Responsiveness of health system is a measure of how the system performs relative to non-health aspects (e.g. choice of provider, client orientation) thus meeting or not meeting the population’s expectations of how it should be treated by providers of care. Source: World Health Report 2000.
Macrolide-R S. pneumoniae(%):Culture Determinants This is where a large graphic or chart can go. Power distance is a measure of the interpersonal power or influence between two individuals when one is the subordinate of the other. Uncertainty avoidance is a measure of tolerance to ambiguous situations, which leads some individuals to feel more pressed for action than others. Masculinity is a measure of the implications that differences between the sexes should have for the emotional and social roles of the genders. Individualism is a measure of the relation between the individual and the collectivity that prevails in a society and is reflected in the way people live together. Long-term orientation is based on the long-term aspects of Confucius thinking: persistence and thrift to personal stability, and respect for tradition. Source: HOFSTEDE.
Summary • Determinants positively correlated with MRSP prevalence: • Use of macrolides and other antibiotic classes (e.g., cephalosporins) • Misuse of antibiotics (low compliance, self-medication with antibiotics) • Factors facilitating cross-transmission of MRSP (having children at home, attendance of daycare, foreign travel) • Determinants negatively correlated with MRSP prevalence: • Use of narrow-spectrum penicillins • Protection against infectious diseases (breastfeeding, general vaccination coverage of infants, and physical activity of adults) • Responsiveness of the health system • No correlation at the macro-level for several determinants that were presented as hypotheses (e.g., population density, socio-economic status)
Discussion & Conclusions • A substantial part of the problem is certainly due to antimicrobial use! • Hypotheses should be tested in future research • Problem of multiple statistical testing • Further multivariate analyses will be performed • Several determinants already appear as candidates for confirmatory studies at the patient level and potential targets for interventions in countries with high prevalence of MRSP: • Increase breastfeeding and immunization coverage • Decrease daycare attendance in early life (< 1y) • Decrease self-medication and OTC sales • Decrease non rational use of macrolides