Download
1 / 56
830 likes | 1.69k Views
ULTRASOUND OF INFERIOR VENA CAVA. OBJECTIVES. Describe indications for using ultrasound at the bedside to image the inferior vena cava. Describe how to performing bedside ultrasound of the inferior vena cava. Use the findings on ultrasound to guide assessment of intravascular volume status.

E N D
OBJECTIVES Describe indications for using ultrasound at the bedside to image the inferior vena cava. Describe how to performing bedside ultrasound of the inferior vena cava. Use the findings on ultrasound to guide assessment of intravascular volume status. Generate group discussion regarding the potential value of learning this procedure for patient management
CASE 46 M was admitted with alcoholic hepatitis and newly diagnosed cirrhosis with ascites. On exam he had flat JVD in supine position, tense abdominal distension, and moderate leg edema to the knees. He was started on a 28 day Trental protocol Hospital Course Day 1-9 - 3 paracenteses; - removal of 11 liters of ascitic fluid. Day 10 - JVD flat in supine position - Abdomen still distended but not tense - moderate leg edema - Na = 136, Cr = 1.0, BUN = 11 - furosemide started at 20 mg QD - spironolactone started at 50mg QD.
CASE Day 12 - JVD flat in supine position - persistent leg edema - apparent increase in abdominal girth on exam - Na = 134, Cr = 0.7, BUN = 12 - furosemide increased to 40mg QD Day 19 - JVD flat in supine position - persistent leg edema - abdominal girth same to slightly decreased - Na = 136, Cr = 0.8, BUN = 12 - furosemide increased to 80mg QD - spironolactone increased to 200mg QD
CASE Day 21 - JVD flat in supine position - leg edema the same - Abdominal girth the same - Na = 130, Cr = 0.9, BUN = 10 Day 24 - JVD flat in the supine position - leg edema the same - Abdominal girth the same to slightly increased - Na = 127, Cr = 0.7, BUN = 13, Urine Na < 10 Daily weights and Input/Output measures were collected sporadically and could not be assessed for any trends.
CLASSIC HYPONATREMIA Hypovolemic Euvolemic Hypervolemic UNa UOsm > SOsm UNa > 40 UNa < 10 > 20 YES NO < 10 > 20 Volume Depletion Mineralcorticoid Deficiency SIADH OTHER Cirrhosis Nephrosis CHF CKD Fluid Restriction plus Diuretics Volume Replacement Fluid Restriction
QUESTION What type of hyponatremia does this patient have and how should it be managed? Hypovolemichyponatremia stop diuretics; begin normal saline infusion; liberalize po fluid intake; monitor Na over the course of the next several days; if Na does not improve or worsens, entertain hypervolemichyponatremia as the cause Hypervolemichyponatremia increase the diuretics and tighten the fluid restriction; monitor Na over the course of the next several days; if Na does not improve or worsens, entertain hypovolemichyponatremia as the cause. Not sure consult nephrology for an opinion about the hyponatremia
INDICATIONS IVC Ultrasound Spontaneously Breathing Mechanical Ventilation Volume Status / CVP Fluid Responsiveness
INDICATIONS Assessing Intravascular Volume Status / CVP • VOLUME DEPLETED STATES • - Hyponatremia • Acute Kidney Injury (? Prerenal) • Diuretic therapy • Sepsis • VOLUME OVERLOAD STATES • Hyponatremia • Heart Failure • Cirrhosis with ascites • Anasarca
INDICATIONS Assessing Fluid Responsiveness in Shock - IVC diameter does not correlate with right atrial pressure in patients who are intubated with shock - Measuring the variation in IVC diameter in these situations can help determine whether the patient’s blood pressure will respond to fluids or whether inotropic support (i.e. dobutamine) will be needed
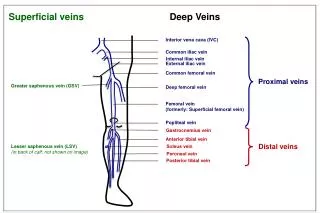
Anatomy The inferior vena cava returns blood from the body to the right atrium Formed by the convergence of the illiac veins Retroperitoneal Right of the aorta Normal size <2.5 cm Varies w respiration
Respiratory variation Expands w/ expiration Contracts w/ inspiration Due to changing intrathoracic pressures.
Respiratory Variation Figure 2: Physiological respiratory variations in IVC diameter in a healthy volunteer breathing quietly.: From: http://www.pifo.uvsq.fr/hebergement/webrea/index.php?option=com_content&task=view&id=36&Itemid=93 IVC diameter decreases on each inspiration. http://www.criticalecho.com/content/tutorial-4-volume-status-and-preload-responsiveness-assessment
Measuring the IVC Diameter Measure IVC 2cm distal to right atrium
CAVAL INDEX (CI) maximum (expiratory) diameter minimal (inspiratory) diameter CI = maximum (expiratory) diameter
CAVAL INDEX (CI) 0% 100% Volume Overload Volume Depletion
PROCEDURE Positioning • Supine • Degree of head elevation has not been shown to make a significant difference in measurements
PROCEDURE • Probe Selection • Low frequency 2-5 MHz • Curvalinear probe
PROCEDURE Approach #1 – Xiphoid View
PROCEDURE Landmarks Aproach #1 – Xiphoid View • Most common approach • Place probe longitudinally just below the xiphoid process with the probe marker to the patient’s head • Look for IVC going into right atrium – may need to move probe 1-2cm to patient’s right and then tilt it slightly towards the heart
PROCEDURE Approach #2 – Anterior Mid-Axillary View
PROCEDURE Landmarks Aproach #2 – Anterior Mid-Axillary View • Place probe longitudinally in right anterior mid-axillary line with marker towards the head • Look for IVC running longitudinally adjacent to liver crossing the diaphragm. • Track superiorly until it enters right atrium confirming that it is the IVC and not the aorta.
PEARLS Bowel Gas • May impede visualization in the xiphoid view • Gentle graded pressure may help move bowel out of way • Don’t press too hard or will collapse IVC causing false measurements • Consider anterior mid-axillary view
PEARLS Plethoric (dilated/sluggish) IVC • Volume overload • Cardiactamponade • Mitral regurgitation • Aorticstenosis
PEARLS Mechanical Ventilation • Causes reversal of IVC changes with respiration • Maximum diameter with inspiration, minimum diameter with expiration
Aorta Thick, echogenic walls Pulsatile High flow velocity Not compressable No respiratory variation Above vertebral bodies IVC Thin walls Usually not pulsatile Low flow velocity Compressable Respiratory variation Right of vertebral bodies PEARLS • IVC v Aorta
SonoSite 180 Plus Changing and Inserting the Transducer
SonoSite 180 Plus Insert the transducer Twist lock counterclockwise
SonoSite 180 Plus Fold lock down
SonoSite 180 Plus Ready to power-up machine
SonoSite 180 Plus Power Button
SonoSite 180 Plus • Wrong Transducer is Connected • Correct Transducer Menu • GYN • OB • Abdominal
SonoSite 180 Plus 2D View (default) M-Mode
SonoSite 180 Plus GAIN Changes the contrast on the screen