Download
1 / 57
670 likes | 1.8k Views
Hypersensitivity. Dr. Prakash Nagarkatti Associate Dean for Basic Science 733-3180 pnagark@uscmed.sc.edu. Allergic condition. Estimated number affected (million). Allergic rhinitis. 19.6. Chronic sinusitis. 32.5. Contact dermatitis & eczema. 5.8. Skin rashes. 12. Asthma. 9-12.

E N D
Hypersensitivity Dr. Prakash Nagarkatti Associate Dean for Basic Science 733-3180 pnagark@uscmed.sc.edu
Allergic condition Estimated number affected (million) Allergic rhinitis 19.6 Chronic sinusitis 32.5 Contact dermatitis & eczema 5.8 Skin rashes 12 Asthma 9-12 Anaphylaxis 1-2 Impact of allergic diseases
Types of Hypersensitivity • Excessive immune response in a sensitized individual leading to tissue damage. • Types of Hypersensitivity: • Types I,II,III------>Immediate, Abs. • Type IV ------>Delayed, T cells.
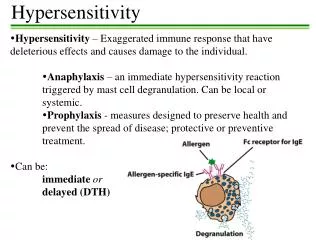
Type II Type I Four types of Hypersensitivity Reactions Ag Target cell Y Y Y Y IgG IgE Target cell Fc receptor Fc recep- tor Killer cell Y Mast cells Ab Histamine Complement Type III Type IV Ag Ag Y Complement Y Th Th cell Endothelial cells Ab Macrophage Y Y Cytokines Neutrophils Activated Macrophage
Type I or Immediate Hypersensitivity Anaphylaxis: Repeat Inj. 2 Weeks later Egg Albumin Dies from asphyxia
Guinea Pig dies from anaphylaxis. Egg albumin IgE Abs Mast cells Histamine • Bronchoconstriction • Vasodilation Lungs
Vasodilatation: Endothelial cells Loss of intravascular fluid Shock Epinephrine Life saving drug.
B cell IL13 TH2 Newly synthesized mediators Sensitization against allergens and type-I hypersensitivity Plasma cell IgE Histamine, tryptase, kininegenase, ECFA Mast cells Leukotriene-B4, C4, D4, prostaglandin D, PAF
Alternate Pathways of Mast Cell Activation Y Y Complement C3a, C5a Anaphylotoxins IgE Fc Receptor Mast cells Histamine Drugs (calcium ionophore, codeine, morphine, mellitin, In addition to the traditional immunological mechanism of Mast cell activation , they can also be activated through alternative pathways that bypass IgE. The common feature in each case is the influx of Calcium ions which triggers mast cell degranulation and release of mediators.
Summary of Mast cell activation Y Y IgE Fc Receptor Mast cells Histamine granule release activated phospholipase A2 arachidonic acid cyclo-oxygenase pathway lipoxygenase pathway histamine,proteolytic enzymes, heparin, chemotactic factors prostaglandins leukotrienes Preformed Mediators Newly Synthesized
Chemo-attractants Physiological Effects of mast cell mediators Attract neutrophils, eosinophils, monocytes and basophils NCF ECF LTB4 Y Y IgE Fc Receptor Activators Mast cells Histamine PAF Tryptase Kininogenase vasodilatation & vascular permeability Histamine and other mediators Microthrombi Activation of C Kinins-->vasodilatation spasmogens Bronchial smooth muscle contraction, mucosal oedema, mucus secretion Histamine Prostaglandins Leukotrienes
Clinical Examples • Hay fever and Asthma----To pollen, house dust, pets etc. • Urticaria(Hives)---Drugs,food. Reddening and itching of skin. • Systemic anaphylaxis---Inj. of Penicillin,Insect bites.
List of Allergens • Grasses/Pollens • Weeds • Foods-->Crab, shrimp, potato, tuna etc • Epidermals--> dog,cat, mouse • Insect bites • House dust • Molds • Drugs
Anaphylaxis to bee venom Bee venom has Mellitin which can directly trigger mast cells
Dust mite fecal pellet
Mediators of allergic reaction: • Allergens: • Proteins or Haptens bound to proteins. • Trigger IgE • IL-4, IL-5, IL-13 and Th2 response.
IgE Abs • 2) IgE: • Only Ab that can bind mast cells. • Cross linking of IgE Fc receptors leads to Mast cell degranulation.
IgE levels in immediate hypersensitivity • Atopic diseases • allergic asthma • allergic eczema • hay fever Helminthic (worm) infections IgE • Immunodeficiency • hyper-IgE syndrome • Wiscott-Aldrich syndrome Miscellaneous diseases • Bronchopulmonary • aspergillosis • IgE myeloma
β-agonist (epinephrine, isoproterenol) α-blocker (phenoxybenzamine) Phosphodiasterase inhibitor (theophylline) α-agonists phenyl epinephrine, nor-epinephrine β-blocker (propanolol) Allergy symptoms and cAMP cAMP Relief from symptoms Worsening of symptoms
Treatments for allergy • Symptomatic Receptor blockers antihistamine, antileukotriene Bronchodialators β-agonists (inhahants) • Prevent mast cell degranulation Ca influx inhibitor (chromolyn sodium) Phosphodiesterase inhibitor (theophylline) • Immunotherapy • Hyposensitization • Anti-IgE(Fc) Ab
Gut Lumen parasitic worm Y Role of IgE in parasitic worm infections Y Soluble Ag Y gut mucosa Y Eosinophils Y B cells Y IgE Mast cells Histamine & other mediators Y APC B cells Y Th cells
Examples of drug-inducedtype II hypersensitivity • Red cells: Penicillin, chloropromazine, phenacetin • Granulocytes: Quinidine, amidopyridine • Platelets: sulphonamides, thiazides
Blood Group Ags Ag Blood Group Ab A A anti-B B B anti-A AB A&B None O ---- anti-A& anti-B Abs against blood group Ags are naturally present and are IgM type.
Transfusion Reaction: +Complement IgM RBC cell lysis Fc K RBC Result: Anaphylactic Shock due to Complement activation.
Hemolytic Disease of the New Born RhD-ve mother Anti-RhD Abs RhD +ve fetus RhD +ve fetus
If mother and fetus have different blood groups, hemolytic disease does not occur. ‘A’ blood group mother Anti-B Abs ‘B’ blood group fetus
Child with Hemolytic Disease • Mother is Rh- and fetus is Rh+. • Fetal RBC entering mother, will trigger anti- Rh Abs. • Such Abs cross placenta and can destroy fetal RBC.
Prophylaxis (RhoGAM) Anti-RhD Abs RhD-ve mother RhD +ve fetus RhD +ve fetus Mid-term injection of RhoGAM and a second injection within a few days of delivery
Prophylaxis Inject Anti-RhD Abs mothers immediately after delivery Prevents sensitization
Type III Hypersensitivity Immune complexes not cleared Activation of Complement C3a & C5a Inflammation Mast cells
antigen cause site of deposition persistent infection bacterial, viral, parasitic, etc. infected organ, kidney mold, plant or animal antigen lung inhaled antigens serum injected material kidney, skin, arteries, joint autoimmunity self antigen kidney, joint, arteries, skin Types of immune complex disease
Type IV Hypersensitivity • Mediated by T cells • Delayed, takes 24-48 hours • Examples: • 1) Contact Hypersens: • Nickel • Chromate • Poison Ivy
Mechanism of Type IV Hypersens. poison Ivy skin Mo urushiol serum protein Inflammation APC Th1
Tuberculin-type Hypersensitivity • Tuberculosis Patient • PPD(Ag derived from M.tuberculosis) • Erythema & Induration • Used as a diagnostic Test • Not accurate.
Role of DTH in Infection: Plays a major role in acute infections caused by intracellular pathogens. Ex: Listeria, Salmonella, Brucella Th1 Macrophage