Download
1 / 86
860 likes | 934 Views
Learn about hypersensitivity or allergy as an immune response inducing exaggerated reactions harmful to the host. Discover its types, mechanisms, manifestations, and detection methods, along with treatment and prevention strategies.

E N D
Hypersensitivity Dr. Rouchelle Tellis M.D, PGDBE, FIME Assoc Prof, Microbiology Yenepoya Medical College
Hypersensitivity or Allergy: Immune response resulting in exaggerated or inappropriate reaction harmful to the host There will be typical clinical manifestations depending on the specific antigen to which the person is hypersensitive. First contact sensitizesthe individual thereby inducing antibody formation. Subsequent contacts elicit allergic response.
Coombs and Gel classified hypersensitivity into 4 main types-I, II, III: antibody mediated Type IV-cell mediated. Recently type V & VI are explained. Antibodies involved for Type I is IgE, Type II & III IgG, IgM & complement is involved. Types I, II, III are immediate types Type IV is considered as Delayed type (DH) where T-cells, Lymphokines & macrophages are involved.
Type I – Atopy, Anaphylaxis – IgE mediated Type II – Cytotoxic – IgG mediated with complement Type III – Immune complex – Arthus phenomenon, serum sickness – IgG and complement Delayed / Type IV – Tuberculin type, contact dermatitis type – T cell, lymphokines, phagocytes.
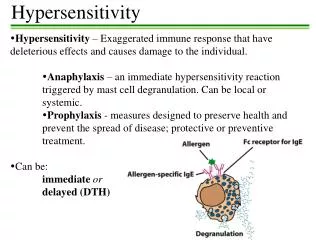
Type I hypersensitivity [Anaphylaxis] HALLMARK OF TYPE I HYPERSENSITIVITY: is production of IgE by sensitized B cells following contact with an allergen which in turn induces mast cell degranulation • Subsequent release of several mediators of inflammation – eg. Histamine • Initiation of the process starts when an antigen or hapten induces the formation of IgE antibody.
IgE binds firmly with its Fc portion to basophils & mast cell surface. Re-exposure to the same antigen results in cross linking of cell bound IgE De-granulation and release of pharmacologically active mediators within minutes [this is immediate phase]
Mechanism of type I hypersensitivity • Two phases: • Sensitization phase • Effector phase Sensitization phase: occurs when individual exposed to the sensitizing or priming dose of Ag for the first time (parenteral route) • Leads to production of sensitized Mast Cells (coated with IgE) waiting for further exposures
Effector phase • When same allergen introduced subsequently ( shocking dose) : directly encounter with IgE- • IgE cross linkage ------ de-granulation of mast cells
Cyclic nucleotides and calcium play essential role in release of mediators. Increase in cyclic GMP within these cells increases mediator release PRIMARY MEDIATORS OF TYPE I HYPERSENSITIVITY:
Manifestations of type I reaction Immediate manifestations: • SYSTEMIC ANAPHYLAXIS • LOCAL ANAPHYLAXIS (Atopy): Allergic rhinitis, asthma, food allergy, atopic dermatitis, drug allergy • Late
Systemic anaphylaxis: • Acute emergency condition: severe dyspnea, hypotension, vascular collapse • Within minutes of exposure to allergen • Bee sting, penicillin, seafood, • Adrenaline is drug of choice
Symptoms – edema and erythema [Wheal & flare] and itching appear rapidly because mediators like histamine are preformed.
Clinically – type I hypersensitivity can appear as urticaria or hives, eczema, rhinitis and conjunctivitis also called hay fever. Clinical manifestation mostly depends on route of entry of allergen. It also depends on location of the mast cells bearing the IgE specific for allergen.
ATOPY : limited to a target tissue or tissue or organ eg. Hay fever, asthma, eczema and urticaria are immediate hypersensitivity reaction. Strong familial disposition. Associated with increased IgE levels. Mechanisms – Failure of regulation of T cell levels [e.g. Increased IL-4 leads to increased IgE synthesis] Enhanced uptake and presentation of environmental antigens Hyper reactivity of target tissues
Atopy can be transferred by serum because antibody mediated. This was used before to diagnose passive cutaneous anaphylaxis called Prausnitz Kustner reaction. [PK reaction] Taking serum from patient and injecting into skin of normal person. Some hours later the test antigen is injected into the “sensitized” site. Yields – immediate wheal and flare reaction This is impractical because danger of transmitting certain viral infection.
Target tissues usually may have increase no. of Th-2 cells. Many of us have experienced atopic disorder at some time in our lives.
Radio immunosorbent test (RAST): helpsto identify the specific IgE against potential offending allergens by Radio allergen sorbent tests. We have to inject suitable specific antigens to the person i.e., in-vitro test and later look for the IgE by ELISA or RIA
Treatment and prevention- • Includes drugs to counteract the action of the mediators • Maintenance of an airway • Support of respiratory and cardiac function • Epinephrine, antihistaminics, corticosteroids or cromolyn sodium- singly or in combination is given. • (cromolyn sodium- prevents release of mediators like histamine from mast cell granules. • Prevention- identification of allergen by skin test and avoidance of the same.
Asthma: • inhaled β-adrenergic bronchodilators – albuterol • corticosteroids like prednisone also effective • Aminophylline – bronchodilator • Monoclonal Ab- anti IgE: effective in clinical trials • Preventing asthma attack: Leukotriene antagonists – e.g. montelukast and cromolyn sodium • -
Allergic rhinitis- antihistamines along with nasal decongestants Allergic conjunctivitis- eye drops containing antihistamines or vasoconstrictors effective Avoiding of inciting allergens like pollens is helpful DESENSITIZATION can be helpful.
Drug hypersensitivity • Drugs (antimicrobial agents, local anesthetics e.g. Penicillin, Lignocaine) can cause hypersensitivity • Usually the metabolic product of the drug acts as a HAPTEN induces antibody formation & elicits immune response. • The IgE so generated can react with the drug or hapten and elicit type I hypersensitivity • Some drugs may be involved in type II and type III reaction.
Drug reaction: rashes, fevers or local or systemic anaphylaxis of varying severities. Before giving penicillin injection or LA or any drug, a careful history of allergy is to be asked. Before injecting perform the skin test (TEST DOSE)
Type II: cytotoxic hypersensitivity • ANTIBODIES produced by the immune response bind to ANTIGENS on the patient's own cell surfaces • Antigens recognized: • INTRINSIC ("self" antigen) or • EXTRINSIC (adsorbed onto the cells during exposure to some foreign antigen as part of infection with a pathogen) • IgG or IgM attach to the antigen by Fab region and acts as a bridge to complement with its Fc portion.
Eg: Abs produced against membrane Ags • Red blood cells in Haemolytic Anaemia • Immune thrombocytopenia • Acetylcholine receptors in Myasthenia Gravis • TSH receptors in Grave's Disease • Goodpasture's syndrome (BM -collagen type IV) in the lung and kidney, attacked by one's own Abs) [2]
Another form of type II hypersensitivity is called ADCC: Antibody dependent cell mediated cytotoxicity: Hyper acute graft rejection
Some infections e.g. Mycoplasma pneumoniae can induce Abs that cross react with RBC antigens – leading to hemolytic anemias.
Type III-Immune- complex hypersensitivity • Occurs when Ag-Ab complexes induce an inflammatory response in tissues • Usually these immune complexes are scavenged by the reticulo- endothelial systems, but occasionally they persist and are deposited in the tissues leading to many disorders.
C/F emerge a week following initial antigen challenge, when the deposited immune complexes can precipitate an inflammatory response • Vasculitis, glomerulo-nephtitis & arthritis are commonly assoc conditions • Observed under Histopathology: as acute necrotizing vasculitis within the affected tissues with neutrophilic infiltration & eosonophilic • Immunofluorescence microscopy to visualize immune complexes
In persistent viral or bacterial infections like Hepatitis B, immune complexes maybe deposited in organs like kidneys and result in damage In auto-immune disorders “self” antigens may elicit Abs that bind to organ antigens or deposit in organs as complexes PMNLs are attracted to the site and hence inflammation and tissue injury occur.
Examples of typical type III reactions include- ARTHUS REACTION- inflammation due to deposition of immune complexes at localized site mainly in the vascular walls, serosa (pleura, pericardium, synovium) and glomeruli.First the animal is injected with antigen repeatedly till they have a high level of IgG Ab. Second the same antigen is injected subcutaneously or intradermally