Download
1 / 28
280 likes | 471 Views
Models of sexual response. Stimuli for arousal Kaplan Masters and Johnson Other models. What is sexual response?. Sexual arousal has both subjective and physiological components. Subjectively, sexual arousal is how aroused people believe or say they are.

E N D
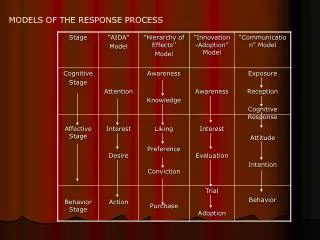
Models of sexual response Stimuli for arousal Kaplan Masters and Johnson Other models
What is sexual response? • Sexual arousal has both subjective and physiological components. • Subjectively, sexual arousal is how aroused people believe or say they are. • Physiological arousal is measured as extent of physiological response, especially vasocongestion.
Animal models • These are not the best models for human sexual response • Order differences: birds, bees, and mammals • Mammal differences: estrous vs. menstruating • Human distinctives: tools, language, war, opposable thumbs…
Gender differences in arousal • For men, there is “a very high correlation between erectile response and how aroused they say they are.” (Cindy Meston, 2003) • For women, such correlations are low to non-existent. • One reason for the difference may be that men are more attentive to physiological sensations than women.
Triggers of sexual response:Activating effect • External: • Stimulated sensations • Pheromones • Drugs • Internal: • Brain centers • Learning and socialization • Personal goals • Cognitive interpretations and attributions
Sensation triggers: Releasing cues? • “Men are turned on by sight, women by touch.” Is that true? • Primary triggers: Touch—or is it meaning? • Are visual stimuli conditioned? • Physiological arousal to gender of stimuli distinguishes heterosexual from homosexual men. • But women respond genitally the same way to stimuli of all gender combinations, regardless of the women’s sexual orientation (Bailey, 2003).
More on sensation triggers • Sounds: A lover’s voice, poetry, music, seductive speech, sex sounds • Tastes and odors: food and drink, perfumes, body cues
Pheromones and reproduction • Lee-Boot effect: Slow and stop estrous • Whitten effect: Synchronize estrous • Vandenbergh effect: Early puberty • Bruce effect: Spontaneous abortion • Synchronized menstrual cycles in college women (McClintock, 1971; Preti et al., 1986) • Underarm sweat and menstrual synchrony (Stern & McClintock, 1998; Cutler, 1999)
Pheromones and attraction • Doty et al. (1975): Odors of vaginal secretions rated as unpleasant by both men and women…but less so around ovulation • Androstenol necklaces increased women’s social interactions with men, but had no effect on men (Cowley & Brooksbank, 1991) • Human vomeronasal organs can respond to pheromones (Liman, 1999 vs. Morris, 2000)
Hormonal control of arousal • Correlational research • Testosterone is the key circulating hormone • Estrogen is the key cellular hormone • Threshold levels of testosterone are necessary for sexual interest in both genders • But testosterone is not a sufficient cause for sexual activity. • Social factors are far more important.
Ovarian hormones and arousal • In primates, ovarian hormones do not control the ability to mate. • Most studies find little or no effect of circulating ovarian hormones on sexual behavior. • However, female monkeys who can control their sexual activity engage in sexual activity at peak estradiol times.
More on ovarian hormones • Human women studied are almost all married. In marriage, other factors than estradiol influence sexual behavior. • Women on the pill show less variation in sexual interest with the menstrual cycle (Alexander et al., 1990)
Sex hormones • Organizing effects: Species-typical mating postures and actions • Activating effects: motivating sexual behavior, and affecting its frequency and intensity • Loss of hormone production is followed by a slow lessening of sexual interest • Previous sexual experience mitigates the change, however.
0 Drugs and sexual arousal • Folk aphrodisiacs • Chocolate, “The ultimate aphrodisiac” • Ginseng, bull or tiger testicles, rhinoceros horn • Oysters and zinc; damiana and other herbs; fruit • Possibly effective aphrodisiacs • Yohimbine in animal studies, clinical trials • Beware compound products containing tadalafil • Arginine, found in yohimbe tree extract, is a precursor of nitric oxide • Cantharides: WARNING! • Testosterone: WARNING! • Dopamine agonists like bupropion and L-DOPA • Date Rape drugs: Rohypnol and GHB
0 Drugs and sexual arousal • Anaphrodisiacs • Alcohol and Shakespeare • Many medications, especially antidepressants • Sildenafil may reverse the antidepressant’s anaphrodisiac effect for women (Nurnberg, Laurellio, & Hensley, 1999) • Anabolic steroids • Blood vessel constrictors like nicotine • Antiandrogens like Depo-Provera, tobacco smoke
Kaplan’s therapy-based model • Desire phase • Psychological components • Physical sensations • Vasocongestive phase • Increased blood in genital region • Erectile responses and lubrication • Increased muscle tension
Kaplan… • Orgasmic-release phase • Orgasm triggers changes • Reverse of vasocongestive phase
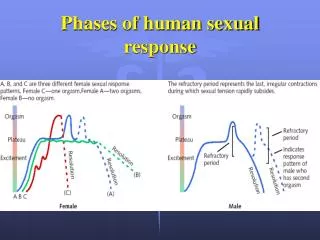
Masters and Johnson’s physiological EPOR model • Excitement phase • Increasing genital response • Erection and transudation • Sex flush • Increasing subjective excitement • Plateau phase • Orgasm or climax • Resolution
Discussion • Are there differences between men and women in the experiencing of any of the phases of the sexual response cycle?
Criticisms of models • Desire phase may be extremely short, or it may be chronic • Plateau experiences are not always found • Continual increase in tension is more often found • The models are biased to the experiences of one gender • Models impose a paradigm on sexual expression
Variations from the pattern • Multiple or absent orgasms • Variation in physical correlates of phases • Orgasm focus • Deception • Refractory period • Coolidge effect • Sexual frustration: Prolonged vasocongestion
Other models of sexual response • Erotic Stimulus Pathway Theory (Reed, 2002) • Seduction: Actions to enhance attractiveness • Sensations: Feelings and thoughts increase arousal • Surrender: Submit to climax • Reflection: What does the experience mean? • FSD-Alert.org
The FSD Manifesto (Tiefer, Tavris, & Hall, 2002) • Challenges the medicalization of women’s sexual problems • 1. Sexual equivalency is denied. • Women do not separate desire from arousal • Women care less about physical than subjective arousal • Women’s sexual complaints are absent from DSM. • Emphasis on equivalency ignores many inequities, such as sexual violence, access to sexual health care, and social environment. • 2. Sexuality is relational, not physiological. • 3. Women are not all the same. • Relational or cultural conflicts, sexual ignorance or fear cause more sexual problems than physical problems, but they go unstudied, in favor of medicalization of problems.
A new classification for problems • I. Sexual problems due to socio-cultural, political, or economic factors • II. Sexual problems relating to partner and relationship • III. Sexual problems due to psychological factors • IV. Sexual problems due to medical factors • Does this classification suggest a different model of sexual response? • Does this analysis fit men better, too?
Aging and sexual response • Reduced and delayed lubrication • Less vasocongestion • Changes dependent on inactivity • Increased likelihood of erectile failure • Delayed orgasm and erection
But the good news is: • Sexual frequency remains unchanged: • In the 20s: Tri-weekly • In the 40s: Try weekly • In the 60s: Try weakly
0 Sandro Botticelli, The birth of Venus, 1485-86
0 Edouard Manet, Le dejeuner sur l’herbe, 1863