Download
1 / 1
10 likes | 177 Views
Physician Inquiry of Secondhand Tobacco Smoke Exposure in Chronic Rhinosinusitis Patients: A Population-Based Case-Control Study. Carrie L. Nieman MD MPH 1 ; Ana Navas-Acien PhD 2 ; Sandra Y. Lin MD 1 ; Douglas D. Reh MD 1,2

E N D
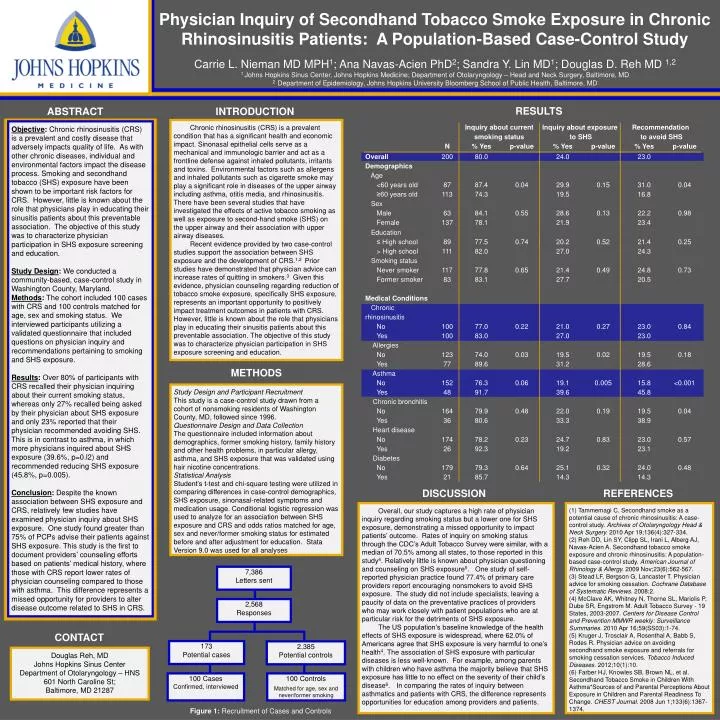
Physician Inquiry of Secondhand Tobacco Smoke Exposure in Chronic Rhinosinusitis Patients: A Population-Based Case-Control Study Carrie L. Nieman MD MPH1; Ana Navas-Acien PhD2; Sandra Y. Lin MD1; Douglas D. Reh MD 1,2 1 Johns Hopkins Sinus Center, Johns Hopkins Medicine; Department of Otolaryngology – Head and Neck Surgery, Baltimore, MD 2 Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD RESULTS ABSTRACT INTRODUCTION Chronic rhinosinusitis (CRS) is a prevalent condition that has a significant health and economic impact. Sinonasal epithelial cells serve as a mechanical and immunologic barrier and act as a frontline defense against inhaled pollutants, irritants and toxins. Environmental factors such as allergens and inhaled pollutants such as cigarette smoke may play a significant role in diseases of the upper airway including asthma, otitis media, and rhinosinusitis. There have been several studies that have investigated the effects of active tobacco smoking as well as exposure to second-hand smoke (SHS) on the upper airway and their association with upper airway diseases. Recent evidence provided by two case-control studies support the association between SHS exposure and the development of CRS.1,2 Prior studies have demonstrated that physician advice can increase rates of quitting in smokers.3Given this evidence, physician counseling regarding reduction of tobacco smoke exposure, specifically SHS exposure, represents an important opportunity to positively impact treatment outcomes in patients with CRS. However, little is known about the role that physicians play in educating their sinusitis patients about this preventable association. The objective of this study was to characterize physician participation in SHS exposure screening and education. Objective: Chronic rhinosinusitis (CRS) is a prevalent and costly disease that adversely impacts quality of life. As with other chronic diseases, individual and environmental factors impact the disease process. Smoking and secondhand tobacco (SHS) exposure have been shown to be important risk factors for CRS. However, little is known about the role that physicians play in educating their sinusitis patients about this preventable association. The objective of this study was to characterize physician participation in SHS exposure screening and education. Study Design: We conducted a community-based, case-control study in Washington County, Maryland. Methods: The cohort included 100 cases with CRS and 100 controls matched for age, sex and smoking status. We interviewed participants utilizing a validated questionnaire that included questions on physician inquiry and recommendations pertaining to smoking and SHS exposure. Results: Over 80% of participants with CRS recalled their physician inquiring about their current smoking status, whereas only 27% recalled being asked by their physician about SHS exposure and only 23% reported that their physician recommended avoiding SHS. This is in contrast to asthma, in which more physicians inquired about SHS exposure (39.6%, p=0.l2) and recommended reducing SHS exposure (45.8%, p=0.005). Conclusion: Despite the known association between SHS exposure and CRS, relatively few studies have examined physician inquiry about SHS exposure. One study found greater than 75% of PCPs advise their patients against SHS exposure. This study is the first to document providers’ counseling efforts based on patients’ medical history, where those with CRS report lower rates of physician counseling compared to those with asthma. This difference represents a missed opportunity for providers to alter disease outcome related to SHS in CRS. METHODS 7,386 Letters sent Study Design and Participant Recruitment This study is a case-control study drawn from a cohort of nonsmoking residents of Washington County, MD, followed since 1996. Questionnaire Design and Data Collection The questionnaire included information about demographics, former smoking history, family history and other health problems, in particular allergy, asthma, and SHS exposure that was validated using hair nicotine concentrations. Statistical Analysis Student’s t-test and chi-square testing were utilized in comparing differences in case-control demographics, SHS exposure, sinonasal-related symptoms and medication usage. Conditional logistic regression was used to analyze for an association between SHS exposure and CRS and odds ratios matched for age, sex and never/former smoking status for estimated before and after adjustment for education. Stata Version 9.0 was used for all analyses 2,568 Responses 173 Potential cases 2,385 Potential controls 100 Cases Confirmed, interviewed 100 Controls Matched for age, sex and never/former smoking DISCUSSION REFERENCES Overall, our study captures a high rate of physician inquiry regarding smoking status but a lower one for SHS exposure, demonstrating a missed opportunity to impact patients’ outcome. Rates of inquiry on smoking status through the CDC’s Adult Tobacco Survey were similar, with a median of 70.5% among all states, to those reported in this study4. Relatively little is known about physician questioning and counseling on SHS exposure5. One study of self-reported physician practice found 77.4% of primary care providers report encouraging nonsmokers to avoid SHS exposure. The study did not include specialists, leaving a paucity of data on the preventative practices of providers who may work closely with patient populations who are at particular risk for the detriments of SHS exposure. The US population’s baseline knowledge of the health effects of SHS exposure is widespread, where 62.0% of Americans agree that SHS exposure is very harmful to one’s health4. The association of SHS exposure with particular diseases is less well-known. For example, among parents with children who have asthma the majority believe that SHS exposure has little to no effect on the severity of their child’s disease6. In comparing the rates of inquiry between asthmatics and patients with CRS, the difference represents opportunities for education among providers and patients. (1) Tammemagi C. Secondhand smoke as a potential cause of chronic rhinosinusitis: A case-control study. Archives of Otolaryngology Head & Neck Surgery. 2010 Apr 19;136(4):327-334. (2) Reh DD, Lin SY, Clipp SL, Irani L, Alberg AJ, Navas-Acien A. Secondhand tobacco smoke exposure and chronic rhinosinusitis: A population-based case-control study. American Journal of Rhinology & Allergy. 2009 Nov;23(6):562-567. (3) Stead LF, Bergson G, Lancaster T. Physician advice for smoking cessation. Cochrane Database of Systematic Reviews. 2008;2. (4) McClave AK, Whitney N, Thorne SL, Mariolis P, Dube SR, Engstrom M. Adult Tobacco Survey - 19 States, 2003-2007. Centers for Disease Control and Prevention MMWR weekly: Surveillance Summaries. 2010 Apr 16;59(SS03):1-74. (5) Kruger J, Trosclair A, Rosenthal A, Babb S, Rodes R. Physician advice on avoiding secondhand smoke exposure and referrals for smoking cessation services. Tobacco Induced Diseases. 2012;10(1):10. (6) Farber HJ, Knowles SB, Brown NL, et al. Secondhand Tobacco Smoke in Children With Asthma*Sources of and Parental Perceptions About Exposure in Children and Parental Readiness To Change. CHEST Journal. 2008 Jun 1;133(6):1367-1374. Figure 1: Recruitment of Cases and Controls. CONTACT Douglas Reh, MD Johns Hopkins Sinus Center Department of Otolaryngology – HNS 601 North Caroline St; Baltimore, MD 21287