Download
1 / 14
140 likes | 526 Views
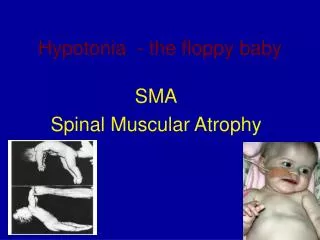
הצגת מקרה . מחלקה נוירולוגית אסף הרופא. A young woman with hypoesthesia of the face. 27-year-old woman, sport teacher Hypoesthesia of the left face and tongue of one month duration Dizziness on getting up in the morning and during body turns

E N D
הצגת מקרה מחלקה נוירולוגית אסף הרופא
A young woman with hypoesthesia of the face • 27-year-old woman, sport teacher • Hypoesthesia of the left face and tongue of one month duration • Dizziness on getting up in the morning and during body turns • No gustatory, visual or hearing symptoms, no limb weakness or sensory changes • Past history: Fe-def. anemia
Examination • Normal visual acuity, normal fundi, no MG • Normal speech • Full eye movements, gaze evoked nystagmus on lateral and up-gaze • Hypoesthesia to pinprick over the left face, mainly cheek and tongue, decreased lt corneal reflex
Examination (cont.) • Normal power, tone and sensation • Lively reflexes in lower limbs • No pathological reflexes • Finger-nose and heel-knee test normal • Normal gait including tandem • Negative Romberg test ???
Auxilliary examinations • Blood tests normal • X-chest ray normal • Carotid duplex normal • Eye exam- normal • Gyn.exam- no evidence of genital ulcers • Audiogram-normal • VEP-normal, SSEP-normal, BERA- latency of wave I normal, prolonged wave III,V latencies ???
CT brain (without contrast): hypodense lesion in the left pons causing compression of the IVth ventricle ???
Brain MRI: Lt vestibular schwannoma
Vestibular schwannoma (VS) • 6% of intracranial tumors • No race or sex predilection • Incidence 10 per million per year (USA, Denmark) • - Sporadic (95%, unilateral, midlife) - associated with NFII (5%,bilat, younger age) - NFI (in 2%, unilateral)
Pathogenesis • VS arises from the Schwann cells of the superior or inferior division of the VN • Most VS arise from the VN at the level of the IAC, just outside the porus • Growth rate- no correlation with gender, symptoms, manifestations or size generally slow (0.1-0.2 cm per year)
Atypical symptoms • Sudden HL - 26% VS, sometimes reversible, but only 1-2% of patients with SHL have VS • Normal hearing – up to 4% VS • Trigeminal neuralgia (but facial hypoesthesia occurs in up to 50% of VS>2cm) • Motor dysfunction of the NV (masseter and lateral temporal muscle atrophy)
Atypical symptoms (cont.) • Facial weakness uncommon, but facial twitching in 10%VS • Intratumoral hemorrhage- triggered by trauma or exercise, - sudden HL, facial spasm, facial sensory disturbances, hoarseness, long tract signs, somnolence • Extratumoral bleeding -SAH
Moffat D: Clinical acumen and VS Am J Otol, 1998, 19: 82-87 • Atypical presentations of VS • 473 patients with VS – 10% atypical presentation – larger tumors, shorter history, better preserved hearing • Facial numbness in 6.4%